Pocket Medicine: The Massachusetts General Hospital Handbook of Internal Medicine (61 page)
Read Pocket Medicine: The Massachusetts General Hospital Handbook of Internal Medicine Online
Authors: Marc Sabatine
Tags: #Medical, #Internal Medicine

BOOK: Pocket Medicine: The Massachusetts General Hospital Handbook of Internal Medicine
7.15Mb size Format: txt, pdf, ePub
• Secondary causes: treat underlying disease • Watch for malnutrition (protein loss), thrombosis (in ~25%, esp. renal vein, b/c loss of ATIII & other endogenous anticoags), infxn (esp. encaps. organisms b/c loss of Ig)
URINALYSIS
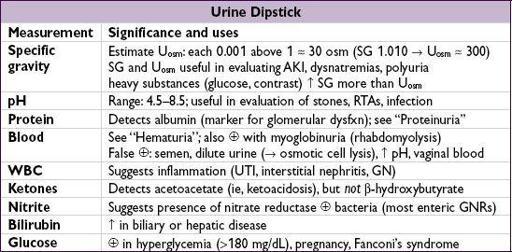
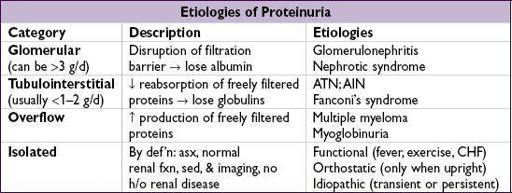
PROTEINURIA
•
Urine dipstick
1+30 mg/dL, 2+
Insensitive for microalbuminuria and myeloma light chains
•
Spot urine
: protein (mg/dL)/creatinine (mg/dL)
NEJM
1983;309:1543) unlike urine dipstick, will accurately measure myeloma light chains reliable surrogate for 24-hr urine, esp. 1st morning void (
JASN
2009;20:436); inaccurate if AKI depends on Cr production, ∴ underestimates if muscular, overestimates if cachectic
•
Microalbuminuria
(30–300 mg/24h
or
mg/L
or
mg/mg of Cr): early sign of glomerular vascular disease; marker for ↑ risk of CV adverse outcomes (
JAMA
2001;286:421)
• Orthostatic proteinuria: typically in adolescents; ~90% of youngwith isolated proteinuria have orthostatic proteinuria; typically resolves spontaneously
HEMATURIA
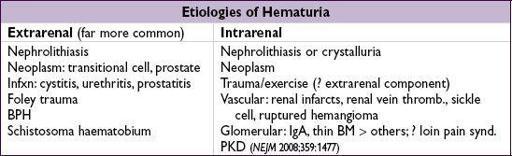
• Wide, overlapping ages for various etiologies, but general guide for common causes:
<20 y: GN, UTI, congenital; 20–60 y: UTI, nephrolithiasis, cancer
>60 y: UTI, cancer
Workup
(
J Urol
2012;188(6 suppl):2473)
•
Urine dipstick
: if ≥3 RBCs;dipstick and
if ≥3 RBCs;dipstick and sediment → myo-or hemoglobinuria •
sediment → myo-or hemoglobinuria •
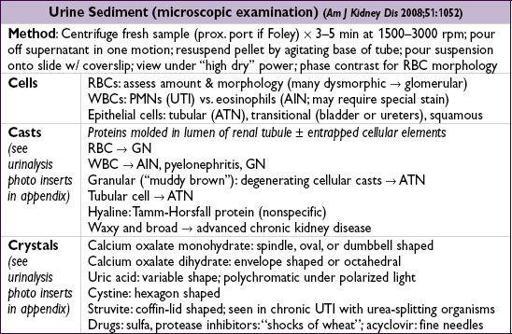
Urine sediment
: dysmorphic RBCs or RBC casts → GN → consider renal bx • If no evidence of glomerulonephritis:
Other books
The Lonely City by Olivia Laing
Luck on the Line by Zoraida Córdova
Trust by Roseau, Robin
Burn (Drift Book 3) by Michael Dean
My Funny Valentine (Pajaro Bay Series Book 4) by Lee, Barbara Cool
Working Girl Blues by Hazel Dickens
Hosker, G [Sword of Cartimandua 05] Revolt of the Red Witch by Griff Hosker
His Every Desire by Shiloh Walker
One Night of Trouble by Elle Kennedy
Tundra by Tim Stevens