Ross & Wilson Anatomy and Physiology in Health and Illness (113 page)
Read Ross & Wilson Anatomy and Physiology in Health and Illness Online
Authors: Anne Waugh,Allison Grant
Tags: #Medical, #Nursing, #General, #Anatomy

The bronchial walls are composed of the same tissues as the trachea, and are lined with ciliated columnar epithelium. The bronchi progressively subdivide into bronchioles (
Fig. 10.17
),
terminal bronchioles
, respiratory bronchioles, alveolar ducts and finally,
alveoli
. The wider passages are called
conducting airways
because their function is to bring air into the lungs, and their walls are too thick to permit gas exchange.
Structural changes in the bronchial passages
As the bronchi divide and become progressively smaller, their structure changes to match their function.
Cartilage
Since rigid cartilage would interfere with expansion of lung tissue and the exchange of gases, it is present for support in the larger airways only. The bronchi contain cartilage rings like the trachea, but as the airways divide, these rings become much smaller plates, and at the bronchiolar level there is no cartilage present in the airway walls at all.
Smooth muscle
As the cartilage disappears from airway walls, it is replaced by smooth muscle. This allows the diameter of the airways to be increased or decreased through the action of the autonomic nervous system, regulating airflow within each lung.
Epithelial lining
The ciliated epithelium is gradually replaced with non-ciliated epithelium, and goblet cells disappear.
Blood and nerve supply, lymph drainage
The arterial supply to the walls of the bronchi and smaller air passages is through branches of the right and left bronchial arteries and the venous return is mainly through the bronchial veins. On the right side they empty into the azygos vein and on the left into the superior intercostal vein (see
Figs 5.41
and
5.42, p. 100
).
The vagus nerves (parasympathetic) stimulate contraction of smooth muscle in the bronchial tree, causing bronchoconstriction, and sympathetic stimulation causes bronchodilation (see
Ch. 7
).
Lymph is drained from the walls of the air passages in a network of lymph vessels. It passes through lymph nodes situated around the trachea and bronchial tree then into the thoracic duct on the left side and right lymphatic duct on the other.
Functions
Control of air entry
The diameter of the respiratory passages is altered by contraction or relaxation of the smooth muscle in their walls, thus regulating the speed and volume of airflow into and within the lungs. These changes are controlled by the autonomic nerve supply: parasympathetic stimulation causes constriction and sympathetic stimulation causes dilation (
pp. 168–169
).
The following functions continue as in the upper airways:
•
warming and humidifying
•
support and patency
•
removal of particulate matter
•
cough reflex.
Respiratory bronchioles and alveoli
Structure
Within each lobe, the lung tissue is further divided by fine sheets of connective tissue into
lobules
. Each lobule is supplied with air by a terminal bronchiole, which further subdivides into respiratory bronchioles, alveolar ducts and large numbers of alveoli (air sacs). There are about 150 million alveoli in the adult lung. It is in these structures that the process of gas exchange occurs. As airways progressively divide and become smaller and smaller, their walls gradually become thinner until muscle and connective tissue disappear, leaving a single layer of simple squamous epithelial cells in the alveolar ducts and alveoli. These distal respiratory passages are supported by a loose network of elastic connective tissue in which macrophages, fibroblasts, nerves and blood and lymph vessels are embedded. The alveoli are surrounded by a dense network of capillaries (
Fig. 10.18
). Exchange of gases in the lung (external respiration) takes place across a membrane made up of the alveolar wall and the capillary wall fused firmly together. This is called the
respiratory membrane
.
On microscopic examination, the extensive air spaces are clearly seen and healthy lung tissue has a honeycomb appearance (
Fig. 10.19
).

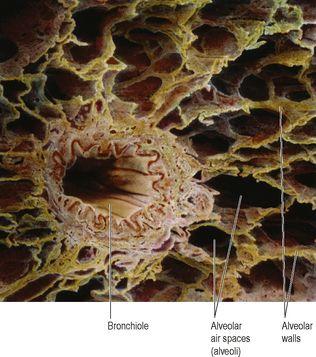
Figure 10.19
Coloured scanning electron micrograph of lung alveoli and a bronchiole.
Lying between the squamous cells are
septal
cells that secrete
surfactant
, a phospholipid fluid which prevents the alveoli from drying out. In addition, surfactant reduces surface tension and prevents alveolar walls collapsing during expiration. Secretion of surfactant into the distal air passages and alveoli begins about the 35th week of fetal life. Its presence in newborn babies facilitates expansion of the lungs and the establishment of respiration. It may not be present in sufficient amounts in the immature lungs of premature babies, causing serious breathing problems.
Nerve supply to bronchioles
Parasympathetic fibres from the vagus nerve cause bronchoconstriction. The absence of supporting cartilage means that small airways may be completely closed off by constriction of their smooth muscle. Sympathetic stimulation relaxes bronchiolar smooth muscle.
Functions
External respiration
(See
p. 250
)
Defence against infection
At this level, ciliated epithelium, goblet cells and mucus are no longer present, because their presence would impede gas exchange and encourage infection. By the time inspired air reaches the alveoli, it is usually clean. Defence relies on protective cells present within the lung tissue. These include lymphocytes and plasma cells, which produce antibodies and phagocytes, including alveolar macrophages. These cells are most active in the distal air passages where ciliated epithelium has been replaced by flattened cells.
Warming and humidifying
These continue as in the upper airways. Inhalation of dry or inadequately humidified air over a period of time causes irritation of the mucosa and encourages infection.
Respiration

Learning outcomes
After studying this section, you should be able to:
describe the actions of the main muscles involved in breathing