Pocket Medicine: The Massachusetts General Hospital Handbook of Internal Medicine (67 page)
Read Pocket Medicine: The Massachusetts General Hospital Handbook of Internal Medicine Online
Authors: Marc Sabatine
Tags: #Medical, #Internal Medicine

BOOK: Pocket Medicine: The Massachusetts General Hospital Handbook of Internal Medicine
2.25Mb size Format: txt, pdf, ePub
>100 mg/dL) and
platelets
; no role for activated protein C in sepsis (
NEJM
2012;366:2055)
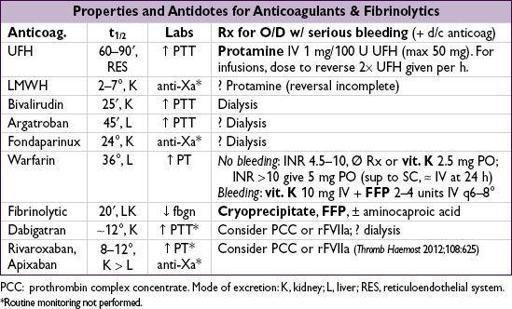
Vitamin K deficiency
• Etiologies: malnutrition, ↓ absorption (
antibiotic
suppression of vitamin K-producing intestinal flora or malabsorption), liver disease (↓ stores),
warfarin
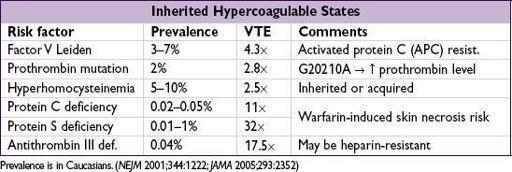
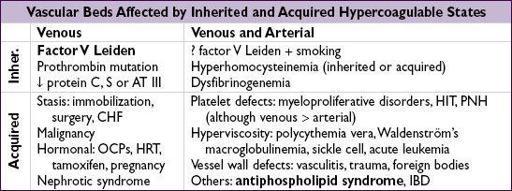
HYPERCOAGULABLE STATES
Suspect in Pts with venous or arterial thrombosis at young age or unusual locations
,
recurrent thromboses or pregnancy loss or FHx
FHx
Diagnostic evaluation
(not routinely required for initial VTE)
• APC resistance screen; prothrombin PCR test; functional assays for proteins C and S, ATIII; homocysteine level; factor VIII levels; anticardiolipin and lupus anticoagulant Ab. Also consider nephrotic syndrome, PNH (esp. if mesenteric thrombus).
• Consider
JAK2
mutation testing if suspect MPN or splanchnic thrombosis.
• Proteins C & S and ATIII levels are affected by acute thrombosis and anticoagulation ∴ levels best assessed ≥2 wk after completing anticoagulation course • Age-appropriate malignancy screening (
Annals
2008;149:323)
Treatment
• Asx w/ inherited risk factor: consider prophylactic anticoag. if develops acquired risk factor • Thrombosis w/ inherited risk factor: see “Venous Thromboembolism”
Antiphospholipid syndrome (APS)
(
J Thromb Haemost
2006;4:295;
NEJM
2013;368:1033)
• Definition: dx requires ≥1 clinical & ≥1 laboratory criteria
Clinical: thrombosis (any) or complication of pregnancy (≥3 spont. abortions before 10 wk or ≥1 fetal loss after 10 wk or premature birth before 34 wk)
Laboratory:
2
-glycoprotein-I (β
2
-GP-I) Ab on ≥2 occasions at least 12 wk apart
• Clinical:
DVT
/
PE
/
CVA
,
recurrent fetal loss
,
thrombocytopenia
, hemolytic anemia, livedo reticularis; “
catastrophic APS
” = ≥3 organ systems in <1 wk w/
Lupus
2003;12:530) → 44% mortality (
Arth Rheum 2006
;54:2568) •
Antiphospholipid antibodies (APLA)
✓
if: SLE, age
<
40 y & arterial thromb, recurrent venous thromb, spontaneous abortion
ACL: Ab against cardiolipin, a mitochondrial phospholipid; IgG more specific than IgM
LA: Ab that prolongs phospholipid-dependent coagulation reactions; ∴ ↑
PTT
that does
not
correct with mixing study but does correct with excess phospholipids or platelets; PT not affected b/c the reaction contains much more phospholipid
β
2
-GP-I: Ab against β
2
-glycoprotein-I, IgG or IgM
False
Clinical significance of different Abs in pathogenesis uncertain
Risk of thromboembolic phenomena may increase with titer of APLs
• Etiologies: primary (idiopathic) or secondary due to
autoimmune syndromes
(eg, SLE),
malignancy
,
infections
, drug reactions • Treatment: UFH/LMWH → warfarin after thromboembolic event (lifelong for most Pts)
Intensity of anticoagulation controversial (
Arthritis Rheum
2007;57:1487)
Initial
venous thrombosis
: INR 2–3 (
NEJM
2003;349:1133;
J Thromb Haemost
2005;3:848)
Initial
arterial thrombosis
: typically INR 2–3 + ASA 81, although some treat to INR 3–4
Recurrent thrombosis
on warfarin: INR 3–4 vs. LMWH (
Arth Rheum
2007;57:1487)
Consider ASA prophylaxis for high-risk asx Pt (eg, SLE)
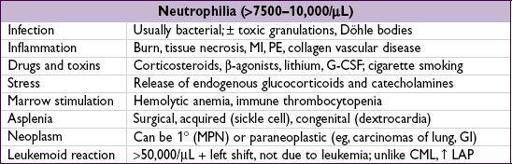
DISORDERS OF LEUKOCYTES
Other books
El quinto jinete by Larry Collins, Dominique Lapierre
Hunter Moran Hangs Out by Patricia Reilly Giff
Her Rancher Bodyguard by Brenda Minton
Broken Play by Samantha Kane
The Devil's Fire by Matt Tomerlin
BEFORE THE PATCH – book one (A Devil Call MC Book) by Fawkes, Ana W.
Mockingbird Songs by Ellory, RJ
Sohlberg and the Gift by Jens Amundsen
The Fray Theory: Resonance by Nelou Keramati
Stalked by Brian Freeman