Pocket Medicine: The Massachusetts General Hospital Handbook of Internal Medicine (83 page)
Read Pocket Medicine: The Massachusetts General Hospital Handbook of Internal Medicine Online
Authors: Marc Sabatine
Tags: #Medical, #Internal Medicine

BOOK: Pocket Medicine: The Massachusetts General Hospital Handbook of Internal Medicine
7.5Mb size Format: txt, pdf, ePub
•
Treatment
: monitor mild disease closely q3–6mo; for severe disease: fluconazole, itraconazole or amphotericin
Blastomycosis (
CID
2008;46:1801)
•
Endemic
: south central, SE and midwest U.S.
•
Clinical manifestations
Acute: 50% subclinical; cough, multilobar PNA; can progress to ARDS
Chronic pulm: cough, wt loss, malaise, CT w/ masses & fibronodular infiltrates
Disseminated: (25–40% of all but >> in immunosupp.): verrucous & ulcerated skin lesions, bone, & GU involvement; CNS rare unless immunosupp.
•
Treatment
: itraconazole (monitor levels); ampho B if severe, disseminated or immunosupp.
Aspergillosis
(
CID
2008;46:327;
NEJM
2009;360:1870)
•
ABPA
;
hypersensitivity pneumonitis
: see “Interstitial Lung Disease”
•
Aspergilloma
: usually in pre-existing cavity (from TB, etc.); most asx, but can lead to hemoptysis; sputum cxin <50%; CT → mobile intracavitary mass with air crescent
Rx: antifungals w/o benefit; embolization or surgery for persistent hemoptysis
•
Necrotizing tracheitis
: white necrotic pseudomembranes in Pts w/ AIDS or lung Tx •
Chronic necrotizing
: seen in COPD, mild immunosupp.; subacute sputum, fever, wt loss; CT: infiltrate ± nodule ± thick pleura; lung bx → invasion •
Invasive/disseminated
: seen if immunosupp. (neutropenia, s/p transplant, steroid Rx, AIDS esp. w/ steroids or neutropenia); s/s PNA w/
chest pain
&
hemoptysis
; CT: nodules, halo sign, air crescent sign; BAL + galactomannan; lung bx if dx inconclusive • Rx (necrotizing/invasive): voriconazole PO preferred to ampho; monitor serum levels
Zygomycetes
(eg,
Mucor
,
Rhizopus
)
•
Epidemiology
:
diabetes mellitus
(70%), heme malignancy, s/p transplant, chronic steroids, deferoxamine or iron overload, trauma, h/o voriconazole Rx or Ppx •
Clinical manifestations
:
rhinocerebral
= periorbital/forehead pain (more extensive than orbital cellulitis), ± fever (may appear nontoxic at first), exophthalmos, ↓ EOM, CNs (V > VII); nasal turbinates ± black eschar but exam can be quite nl. Also,
pulmonary
(PNA w/ infarct & necrosis);
cutaneous
(indurated painful cellulitis ± eschar);
GI
(necrotic ulcers).
•
Treatment
: Serial debridement + ampho (? + posaconazole). High mortality despite Rx.
Fungal diagnostics
•
Culture
:
Candida
grows in blood/urine Cx, but ↓ Se of BCx if deep tissue infection; others (eg,
Crypto
,
Histo
) ↓↓ Se of BCx; if suspect
Coccidio
alert lab
(biohazard)
•
Antibody detection
:
Histo
,
Blasto
,
Coccidio
,
Aspergillus
. Se variable (best for
Coccidio
).
•
Antigen detection
Histo urine/serum Ag
: Se of urine Ag 90% (serum 80%) if dissem; Sp limited by X-react
Crypto Ag
(serum, CSF): serum Ag >90% Se & Sp in invasive infxn, less for pulm only
1
,
3-
b
-D-glucan
: Se for many fungal infxns (
Candida, Aspergillus, Histo, Coccidio, Fusarium, Pneumocystis, Sporothrix
; but
not Crypto, Blasto, Mucor, Rhizopus
); not Sp
Galactomannan
: more specific for
Aspergillus
, but Se <50%. ↑ Se on BAL.
•
Biopsy
(ie, histopathology): nb, no grinding of tissue if Zygomycetes suspected
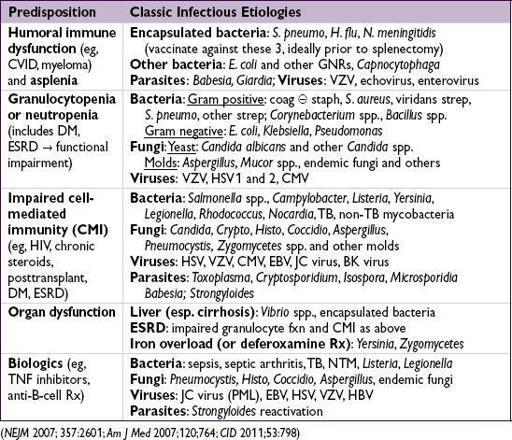
INFXNS IN IMMUNOSUPPRESSED HOSTS
Overview
• Many immunophenotypes, meds or systemic diseases predispose to infection
• Many Pts have ≥1 risk (eg, DM, ESRD, transplant, extremes of age); duration of risk varies
• The following is not an exhaustive list, but a delineation of common or classic etiologies
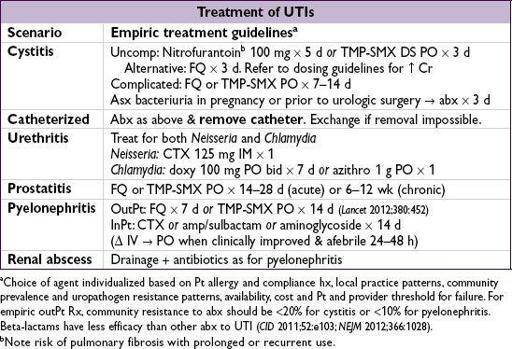
URINARY TRACT INFECTIONS
Definitions
• Anatomic
lower
: urethritis, cystitis (superficial infection of bladder)
upper
: pyelonephritis (inflam of renal parenchyma), renal/perinephric abscess, prostatitis
• Clinical
uncomplicated
: cystitis in immunocompetent nonpregnant women w/o underlying structural or neurologic disease
complicated
: upper tract infection in women
or
any UTI in men or pregnant women
or
UTI with underlying structural disease or immunosuppression
Microbiology
• Uncomplicated UTI:
E. coli
(80%),
Proteus
,
Klebsiella
,
S. saprophyticus
(
CID
2004;39:75). In healthy, nonpregnant women, lactobacilli, enterococci, Group B strep and coag-neg staph (except
S. saprophyticus
) usually contaminants (
Annals
2012;156:ITC3).
• Complicated UTI:
E. coli
(30%), enterococci (20%),
PsA
(20%),
S. epi
(15%), other GNR
• Catheter-associated UTI:
yeast
(30%),
E. coli
(25%), other GNR, enterococci,
S. epi
• Urethritis:
Chlamydia trachomatis, Neisseria gonorrhoeae, Ureaplasma urealyticum, Trichomonas vaginalis, Mycoplasma genitalium
, HSV
•
S. aureus
: uncommon primary urinary pathogen in absence of catheter or recent instrumentation; ∴ consider bacteremia w/ hematogenous seeding
Clinical manifestations
•
Cystitis
:
dysuria
,
urgency
,
frequency
, hematuria, Δ in urine color/odor, suprapubic pain; fever usually
absent
. R/o vaginitis with symptoms of cystitis and urethritis.
•
Urethritis
: similar to cystitis except
urethral discharge
can be present •
Prostatitis
chronic
: similar to cystitis except
symptoms of obstruction
(hesitancy, weak stream)
acute
: perineal pain, fever, tenderness on prostate exam
•
Pyelonephritis
: fever, chills, flank or back pain, nausea, vomiting, diarrhea •
Renal abscess
(intrarenal, perinephric): identical to pyelonephritis w/
persistent fever despite appropriate antibiotics
Diagnostic studies
•
Urinalysis
:
pyuria
+
bacteriuria
± hematuria ± nitrites •
Urine Cx
(from clean-catch midstream or straight-cath specimen): obtain cx only if sx
Significant bacterial counts: typically ≥10
5
CFU/mL in women, ≥10
3
CFU/mL in men or catheterized Pts. Counts may vary depending on dilution & stage of infxn; interpret in context of symptoms and host.
Pyuria &UCx = sterile pyuria → urethritis, nephritis, renal tuberculosis, foreign body
• Blood cultures: obtain in febrile Pts; consider in complicated UTIs • DNA detection/cx for
C. trachomatis/N. gonorrhoeae
in high-risk Pts or sterile pyuria • If ? prostatitis: 1st void, midstream, prostatic expressage & postprostatic massage UCx • Abdominal CT: r/o abscess in Pts with pyelo who fail to defervesce after 72 h • Urologic w/u (renal U/S w/ PVR, abd CT, voiding cystography) if recurrent UTIs in men
SOFT TISSUE AND BONE INFECTIONS
CELLULITIS
Infection of superficial and deep dermis and subcutaneous fat
Microbiology & clinical
(
NEJM
2004;350:904;
CID
2005;41:1373)
• Primarily strep and staph, including MRSA; may include GNRs in diabetics/immunosupp.
•
Community-acquired MRSA (CA-MRSA)
(
NEJM
2005;352:1485 & 2006;355:666)
Other books
Witness by Piper Davenport
Forgotten Awakenings (Awakenings #2) by Lisa Bilbrey
Show Me How to Love (Caldwell Family Book 1) by Synithia Williams
Murder At Murder At the Mimosa Inn, The by Joan Hess
Crashing The Concert (Undercover Lust # 2) by Nicole Sanchez
Zamani by Angelic Rodgers
Várias Histórias by Machado de Assis
Loving what He Wants (Celine and Rhyland Series) by Deorre, Iris
Kept - I've Become His Dirty Little Secret by Jamie Fuchs
Silent City by Alex Segura