Pocket Medicine: The Massachusetts General Hospital Handbook of Internal Medicine (87 page)
Read Pocket Medicine: The Massachusetts General Hospital Handbook of Internal Medicine Online
Authors: Marc Sabatine
Tags: #Medical, #Internal Medicine

BOOK: Pocket Medicine: The Massachusetts General Hospital Handbook of Internal Medicine
11.03Mb size Format: txt, pdf, ePub
Treatment
• Rx if can initiate
w/in 72 h of skin lesions
in healthy Pt or at
any time
in immunosupp.
• Valacyclovir or famciclovir × 7–14 d, or until lesions fully crusted; acyclovir 10 mg/kg IV q8h if dissem. or high-risk Pt (medically ill, immunosupp., V1 zoster w/ ophthalmic s/s, etc.) • Prevention: vaccine approved for Pts >50 y (↓ lifetime risk from 20% to 10%, also ↓ PHN)
BACTERIAL ENDOCARDITIS
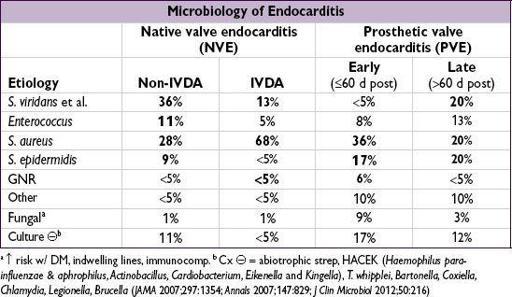
Definition
• Infection of endothelium of heart (including but not limited to the valves) • Acute (ABE): infxn of normal valves w/ virulent organism (eg,
S. aureus
, group A or other β-hemolytic strep,
Strep pneumo
) • Subacute (SBE): indolent infxn w/ less virulent organism (eg,
S. viridans
); often abnl valves
Predisposing conditions
•
Abnormal valve
High risk:
prior endocarditis, rheumatic valvular disease, AoV disease (incl. bicuspid), complex cyanotic lesions, prosthesis (annual risk 0.3–1%)
Medium risk:
MV disease (including MVP w/ MR or leaflet thickening), HCMP
•
Abnormal risk of bacteremia
: IDU, indwelling venous catheters, poor dentition, hemodialysis, DM, intracardiac devices (eg, pacemaker, ICD)
Clinical manifestations
(
Archives
2009;169:463)
•
Persistent bacteremia
:
fever
(80–90%), chills, night sweats, anorexia, wt loss, fatigue •
Valvular or perivalvular infection
: CHF, conduction abnormalities •
Septic emboli
: systemic emboli (eg, to periphery, CNS, kidneys, spleen or joints), stroke,
PE (if right-sided), mycotic aneurysm, MI (coronary artery embolism)
•
Immune complex phenomena
: arthritis, glomerulonephritis,RF, ↑ ESR
•
SBE:
can p/w fatigue, nonspecific sx in Pts w/o risk factors; ∴ need high index of suspicion
Physical exam
• HEENT:
Roth spots
(retinal hemorrhage + pale center),
petechiae
(conjunctivae, palate) • Cardiac:
murmur
(85%),
new
valve regurgitation
(40–85%) ± thrill (fenestrated valve or ruptured chordae), muffled sounds (PV).
Frequent exams
for Δ murmurs, s/s CHF.
• Abdomen: tender splenomegaly; musculoskeletal: arthritis, vertebral tenderness • Extremities (
typically seen in SBE, not ABE
)
Janeway lesions
(septic emboli → nontender, hemorrhagic macules on palms or soles)
Osler’s nodes
(immune complexes → tender nodules on pads of digits)
proximal
nail bed splinter hemorrhages (8–15%); petechiae (33%); clubbing
• Neuro: Δ MS or focal deficits • Devices: erythema, tenderness or drainage at catheter site, PM/ICD pocket tenderness
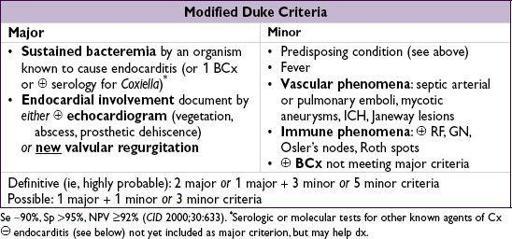
Diagnostic studies
•
Blood cultures
(
before abx
): at least 3 sets (aerobic & anaerobic bottles) from different sites, ideally spaced ≥1 h apart. ✓ BCx (at least 2 sets) after appropriate abx have been initiated to document clearance; repeat q24–48h until.
• CBC w/ diff (↑ WBC common in ABE; anemia in 90% SBE), ESR, RF, BUN/Cr, U/A, & UCx •
ECG
(on admission and at regular intervals) to assess for new conduction abnormalities •
Echocardiogram
: obtain TTE if low clinical suspicion, expect good image quality; TEE if (i) mod-to-high suspicion, (ii) high-risk Pt (prosthetic valve, prior IE, congenital heart dis), (iii) TTE nondx, (iv) TTE
Circ
2005;111:e394)

•
Cx
: may be due to abx prior to BCx. PCR, bacterial 16S ribosomal RNA, serologies may be helpful. Detailed hx: animal exposure, travel, unpasteurized dairy,
etc.
Seek ID eval (
Med
2005;84:162;
NEJM
2007;356:715).
Treatment
(
NEJM
2013;368:1425)
•
Obtain culture data first
ABE → abx should start promptly after cx data obtained
SBE → if Pt hemodynamically stable, may delay abx to properly obtain adequate BCx data, esp. if prior abx used
•
Suggested empiric therapy
(
Circ
2005;111:e394)
native valve ABE
:
vanco
(± gent; no longer routinely recommended)
native valve SBE
:
ceftriaxone
(
or
amp if ? enterococcus; eg, olderor ob/gyn) ±
gent
PVE
:
early
(≤60 d):
vanco + cefepime + gent
;
intermediate
(60–365 d):
vanco
+
gent
;
late
(>1 y):
vanco + CTX + gent
native or prosthetic cx
depends on host & epi
,
seek ID consultation
Other books
Nightshade City by Hilary Wagner
So Over You by Gwen Hayes
Sex, Marriage and Family in World Religions by Browning, Green, Witte
Two Time by Chris Knopf
All of Me (All Series Book 2) by Ann, Natalie
Demons of Lust by Silvana S Moss
Love Redeemed by Sorcha Mowbray
Maxwell's Island by M.J. Trow
Play With Fire by Dana Stabenow
Unfurl by Swanson, Cidney