Pocket Medicine: The Massachusetts General Hospital Handbook of Internal Medicine (22 page)
Read Pocket Medicine: The Massachusetts General Hospital Handbook of Internal Medicine Online
Authors: Marc Sabatine
Tags: #Medical, #Internal Medicine

BOOK: Pocket Medicine: The Massachusetts General Hospital Handbook of Internal Medicine
10.81Mb size Format: txt, pdf, ePub
Cardioversion
• Consider pharm or electrical cardioversion w/ 1st AF episode or if sx;
if AF >48 h, 2–5% risk stroke w/ cardioversion (
pharmacologic or electric
) ∴ either TEE to r/o thrombus or ensure therapeutic anticoagulation for ≥3 wk prior • Likelihood of success ∝ AF duration & atrial size; control precip. (eg, vol status, thyroid) • Consider pre-Rx w/ antiarrhythmic drugs (esp. if 1st cardioversion attempt fails) • For pharmacologic cardioversion, class III and IC drugs have best proven efficacy • If SR returns (spont. or w/ Rx), atria may be
mech. stunned
; also, high risk of recurrent AF over next 3 mo. ∴
Anticoag postcardioversion
≥
4–12 wk
(? unless <48 h and low risk).
Nonpharmacologic therapy
•
Radiofrequency ablation
(circumferential pulm. vein isolation;
Lancet
2012;380:1509): ~80% success; reasonable alternative to AAD in sx persistent or paroxysmal AF w/o ↑↑ LA or ↓ EF (NEJM 2012;367:1587; RAAFT 2, HRS 2012) • Surgical “maze” procedure (70–95% success rate) option if undergoing cardiac surgery • LA appendage closure/resection: reasonable if another indication for cardiac surgery
percutaneous closure noninferior to warfarin, ↓ risk of ICH, but w/ procedural complic; additional studies & approaches underway (Lancet 2009;374:534; PREVAIL, ACC 2013)
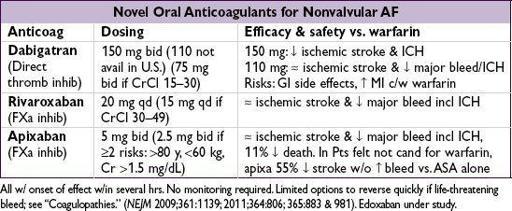
Oral anticoagulation (Chest 2012;141:e531S; EHJ 2012;33:2719; Circ 2013;127:1916)
•
All valvular AF
as stroke risk very high • Nonvalvular AF: stroke risk ~4.5%/y; anticoag → 68% ↓ stroke; use a risk score to guide Rx:
CHADS
2
: CHF
(1 point),
HTN
(1), Age ≥75 y (1), DM (1), prior Stroke/TIA (2)
CHA
2
DS
2
-
VASc
: adds 65–74 y (1), >75 y (2); vasc dis. (1);sex (1)
score
>
2
→
anticoag; score 1
→
consider anticoag
or ASA (? latter reasonable if risk factor 65–74 y, vasc dis. or
•
Rx options
:
factor Xa or direct thrombin inhib
(nonvalv only; no monitoring required) or
warfarin
(INR 2–3; w/ UFH bridge if high risk of stroke); if Pt refuses anticoag, consider
ASA + clopi or, even less effective, ASA alone (NEJM 2009;360:2066)
SYNCOPE
Definition
• Symptom of sudden transient loss of consciousness due to global cerebral hypoperfusion • If CPR or cardioversion required, then SCD and not syncope (different prognosis)
Etiologies
(
NEJM
2002;347:878;
JACC
2006;47:473;
Eur Heart
J
2009;30:2631)
•
Neurocardiogenic
(a.k.a. vasovagal, ~20%;
NEJM
2005;352:1004): ↑ sympathetic tone → vigorous contraction of LV → mechanoreceptors in LV trigger ↑ vagal tone (hyperactive Bezold-Jarisch reflex) → ↓ HR (cardioinhibitory) and/or ↓ BP (vasodepressor)
cough, deglutition, defecation, & micturition → ↑ vagal tone and thus can be precipitants
related disorder: carotid sinus hypersensitivity (exagg vagal resp to carotid massage) •
Orthostatic hypotension
(10%)
hypovolemia/diuretics, deconditioning; vasodilat. (esp. if combined w/chronotropes)
autonomic neuropathy [1° = Parkinson’s, Shy-Drager, Lewy body dementia, POTS (dysautonomia in the young); 2° = DM, EtOH, amyloidosis, CKD] (
NEJM
2008;358:615)
•
Cardiovascular
Arrhythmia
(15%)
Bradyarrhythmias: SSS, high-grade AV block,
Tachyarrhythmias: VT, SVT (syncope rare unless structural heart disease or WPW)
Mechanical
(5%)
Endocardial/Valvular: AS, MS, PS, prosthetic valve thrombosis, myxoma
Myocardial: pump dysfxn from MI or outflow obstruction from HCMP (but usually VT)
Pericardial: tamponade
Vascular: PE, PHT, aortic dissection, ruptured AAA, subclavian steal
•
Neurologic
(10%): seizure (technically not syncope), TIA/CVA, vertebrobasilar
insufficiency, dissection of cerebral arteries, migraine, narcolepsy
• Misc. causes of LOC (but not syncope): hypoglycemia, hypoxia, anemia, psychogenic
Workup
(etiology cannot be determined in
~40% of cases)
•
H&P incl. orthostatic VS have highest yield and most cost effective
(
Archives
2009;169:1299) •
History
(from Pt and
witnesses
if available)
activity and posture before the incident
precipitating factors: exertion (AS, HCMP, PHT), positional Δ (orthostatic hypotension), stressors such as sight of blood, pain, emotional distress, fatigue, prolonged standing, warm environment, N/V, cough/micturition/defecation/swallowing (neurocardiogenic), head turning or shaving (carotid sinus hypersens.); arm exercise (subclavian steal)
prodrome (eg, diaphoresis, nausea, blurry vision): cardiac <~5 sec, vasovagal >~5 sec
associated sx: chest pain, palp., neurologic, postictal, bowel or bladder incontinence (convulsive activity for <10 sec may occur w/ transient cerebral HoTN & mimic seizure)
•
PMH
: prior syncope, previous cardiac or neurologic dis.; no CV disease at baseline → 5% cardiac, 25% vasovagal; CV disease → 20% cardiac, 10% vasovagal (
NEJM
2002;347:878) •
Medications that may act as precipitants
vasodilators: a-blockers, nitrates, ACEI/ARB, CCB, hydralazine, phenothiazines, antidep.
diuretics;
proarrhythmic or QT prolonging: class IA, IC or III antiarrhythmics (see “ECG”)
psychoactive drugs: antipsychotics, TCA, barbiturates, benzodiazepines, EtOH
•
Family history
: CMP, SCD, syncope (vasovagal may have genetic component) •
Physical exam
VS including
orthostatics
(if supine → standing results in >20 mmHg ↓ SBP, >10 mmHg ↓ DBP, or >10–20 bpm ↑ HR), BP in both arms
Other books
Vengeance Trail by Bill Brooks
What Happens in Vegas: A BWWM Alpha Male Romance by Stacey Mills, Cristina Grenier
Beyond Reason by Gwen Kirkwood
Fire Kin by M.J. Scott
How to Survive a Killer Seance by Warner, Penny
Mistress No More by Bryant, Niobia
Borrowed Billionaire #5 Set it on Fire by Strong, Mimi
PERFECT YOUTH: The Birth of Canadian Punk by Sam Sutherland
The Boy is Back in Town by Nina Harrington
Cobalt Blue by Sachin Kundalkar