Ross & Wilson Anatomy and Physiology in Health and Illness (189 page)
Read Ross & Wilson Anatomy and Physiology in Health and Illness Online
Authors: Anne Waugh,Allison Grant
Tags: #Medical, #Nursing, #General, #Anatomy

This ball and socket joint is formed by the cup-shaped acetabulum of the innominate (hip) bone and the almost spherical head of the femur. The capsular ligament encloses the head and most of the neck of the femur. The cavity is deepened by the
acetabular labrum
, a ring of fibrocartilage attached to the rim of the acetabulum, which stabilises the joint without limiting its range of movement. The hip joint is necessarily a sturdy and powerful joint, since it bears all body weight when standing upright. It is stabilised by its surrounding musculature, but its ligaments are also important. The three main external ligaments are the
iliofemoral
,
pubofemoral
and
ischiofemoral
ligaments, which are localised thickenings of the joint capsule (
Fig. 16.51B
). Within the joint, the
ligament of the head of the femur
(
ligamentum teres
) attaches the femoral head to the acetabulum (
Fig. 16.51A
and
C
).
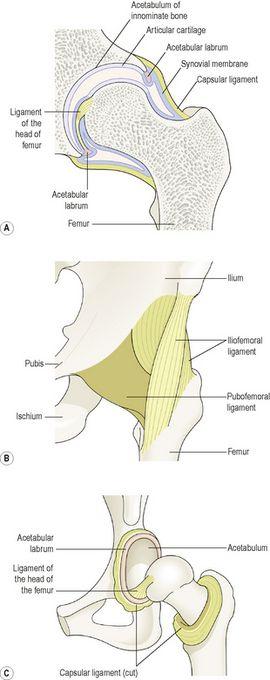
Figure 16.51
The hip joint. A.
Section.
B
. Supporting ligaments.
C.
Head of femur and acetabulum separated to show acetabular labrum and ligament of head of femur.
Muscles and movements (see
Fig. 16.66
)
The lower limb can be extended, flexed, abducted, adducted, rotated and circumducted at the hip joint (
Table 16.5
).
Table 16.5
Muscles and movements at the hip joint
| Flexion | Psoas, iliacus, sartorius |
| Extension | Gluteus maximus, hamstrings |
| Abduction | Gluteus medius and minimus, sartorius |
| Adduction | Adductor group (longus, brevis and magnus) |
| Medial rotation | Gluteus medius and minimus, adductor group |
| Lateral rotation | Gluteus maximus, quadratus femoris, obturators |
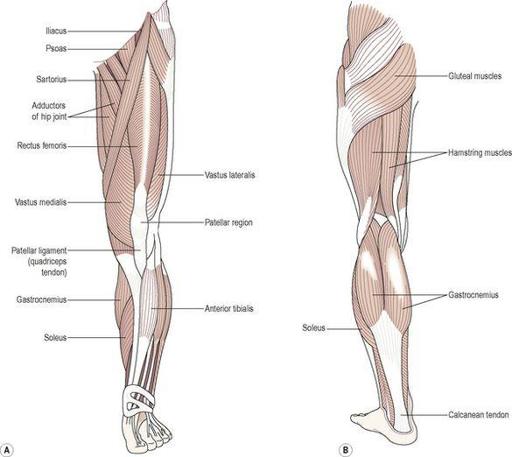
Figure 16.66
The main muscles of the lower limb. A.
Anterior view.
B.
Posterior view.
Knee joint (
Fig. 16.52
)
This is the largest and most complex joint. It is a hinge joint formed by the condyles of the femur, the condyles of the tibia and the posterior surface of the patella. The anterior part of the capsule is formed by the tendon of the quadriceps femoris muscle, which also supports the patella. Intracapsular structures include two
cruciate ligaments
that cross each other, extending from the
intercondylar notch
of the femur to the
intercondylar eminence
of the tibia. They help to stabilise the joint.
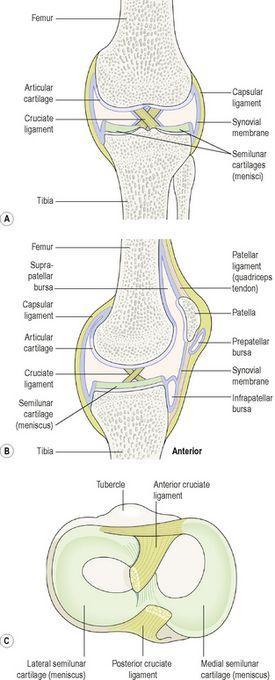
Figure 16.52
The knee joint. A.
Section viewed from the front.
B.
Section viewed from the side.
C.
The superior surface of the tibia, showing the semilunar cartilages and the cruciate ligaments.
Semilunar cartilages
or
menisci
are incomplete discs of white fibrocartilage lying on top of the articular condyles of the tibia. They are wedge shaped, being thicker at their outer edges, and provide stability. They prevent lateral displacement of the bones, and cushion the moving joint by shifting within the joint space according to the relative positions of the articulating bones.
Bursae and pads of fat are numerous. They prevent friction between a bone and a ligament or tendon and between the skin and the patella. Synovial membrane covers the cruciate ligaments and the pads of fat. The menisci are not covered with synovial membrane because they are weight bearing. External ligaments of the joint provide further support, making it a hard joint to dislocate. The main ligaments are the patellar ligament, an extension of the quadriceps tendon, the popliteal ligaments at the back of the knee and the collateral ligaments to each side.
Muscles and movements (see
Fig. 16.66
)
Possible movements at this joint are flexion, extension and a rotatory movement that ‘locks’ the joint when it is fully extended. When the joint is locked, it is possible to stand upright for long periods of time without tiring the knee extensors. The main muscles extending the knee are the quadriceps femoris, and the principal flexors are the gastrocnemius and hamstrings.
Ankle joint (
Fig. 16.53
)
This hinge joint is formed by the distal end of the tibia and its malleolus (medial malleolus), the distal end of the fibula (lateral malleolus) and the talus. There are four important ligaments strengthening this joint: the deltoid and the anterior, posterior, medial and lateral ligaments.
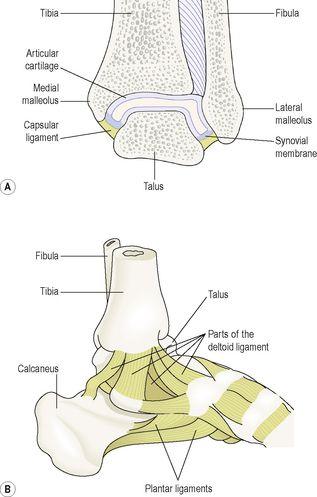
Figure 16.53
The left ankle joint. A.
Section viewed from the front.
B.
Supporting ligaments, medial view.
Muscles and movements (see
Fig. 16.66
)
The movements of
inversion
and
eversion
occur between the tarsal bones and not at the ankle joint. Ankle joint movements and the related muscles are shown in
Table 16.6
.
Table 16.6
Muscles and movements at the ankle joint
| Dorsiflexion (lifting toes towards calf) | Anterior tibialis and toe extensors |
| Plantar flexion (rising on tiptoe) | Gastrocnemius, soleus and toe flexors |
Joints of the feet and toes
There are a number of synovial joints between the tarsal bones, between the tarsal and metatarsal bones, between the metatarsals and proximal phalanges and between the phalanges. Movements are produced by muscles in the leg with long tendons that cross the ankle joint, and by muscles of the foot. The tendons crossing the ankle joint are encased in synovial sheaths and are held close to the bones by strong transverse ligaments. They move smoothly within their sheaths as the joints move. In addition to moving the joints of the foot, these muscles support the arches of the foot and help to maintain body balance.
Muscle tissue

Learning outcomes
After studying this section you should be able to:
identify the main characteristics of skeletal muscle