Ross & Wilson Anatomy and Physiology in Health and Illness (193 page)
Read Ross & Wilson Anatomy and Physiology in Health and Illness Online
Authors: Anne Waugh,Allison Grant
Tags: #Medical, #Nursing, #General, #Anatomy

External oblique
This muscle extends from the lower ribs downwards and forward to be inserted into the iliac crest and, by an aponeurosis, to the linea alba.
Internal oblique
This muscle lies deep to the external oblique. Its fibres arise from the iliac crest and by a broad band of fascia from the spinous processes of the lumbar vertebrae. The fibres pass upwards towards the midline to be inserted into the lower ribs and, by an aponeurosis, into the linea alba. The fibres are at right angles to those of the external oblique.
Transversus abdominis
This is the deepest muscle of the abdominal wall. The fibres arise from the iliac crest and the lumbar vertebrae and pass across the abdominal wall to be inserted into the linea alba by an aponeurosis. The fibres are at right angles to those of the rectus abdominis.
Functions
The main function of these paired muscles is to form the strong muscular anterior wall of the abdominal cavity. When the muscles contract together they:
•
compress the abdominal organs
•
flex the vertebral column in the lumbar region (
Fig. 16.61
).
Contraction of the muscles on one side only bends the trunk towards that side. Contraction of the oblique muscles on one side rotates the trunk.
Inguinal canal
This canal is 2.5 to 4 cm long and passes obliquely through the abdominal wall. It runs parallel to and immediately in front of the transversalis fascia and part of the inguinal ligament (
Fig. 16.60
). In the male it contains the
spermatic cord
and in the female, the
round ligament
. It constitutes a weak point in the otherwise strong abdominal wall through which herniation may occur.
Muscles of the thorax
These muscles are concerned with respiration, and are discussed in
Chapter 10 (p. 247)
.
Muscles of the pelvic floor (
Fig. 16.64
)
The pelvic floor is divided into two identical halves that unite along the midline. Each half consists of fascia and muscle. The muscles are:
•
levator ani
•
coccygeus.
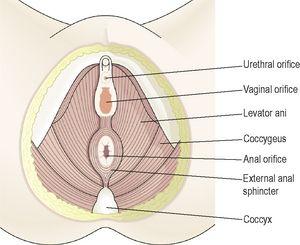
Figure 16.64
The muscles of the female pelvic floor.
Levator ani
This is a pair of broad flat muscles, forming the anterior part of the pelvic floor. They originate from the inner surface of the true pelvis and unite in the midline. Together they form a sling that supports the pelvic organs.
Coccygeus
This is a paired triangular sheet of muscle and tendinous fibres situated behind the levator ani. They originate from the medial surface of the ischium and are inserted into the sacrum and coccyx. They complete the formation of the pelvic floor, which is perforated in the male by the urethra and anus, and in the female by the urethra, vagina and anus.
Functions
The pelvic floor supports the organs of the pelvis and maintains continence, i.e. it resists raised intrapelvic pressure during micturition and defaecation.
Muscles of the shoulder and upper limb (
Fig. 16.65
)
These muscles stabilise the association between the appendicular and axial skeletons at the pectoral girdle, and stabilise and allow movement of the shoulders and upper arms.
Deltoid
These muscle fibres originate from the clavicle, acromion process and spine of scapula and radiate over the shoulder joint to be inserted into the deltoid tuberosity of the humerus. It forms the fleshy and rounded contour of the shoulder and the main function is movement of the arm. The anterior part causes flexion, the middle or main part abduction and the posterior part extends and laterally rotates the shoulder joint.
Pectoralis major
This lies on the anterior thoracic wall. The fibres originate from the middle third of the clavicle and from the sternum and are inserted into the lip of the intertubercular groove of the humerus. It draws the arm forward and towards the body, i.e. flexes and adducts.
Coracobrachialis
This lies on the upper medial aspect of the arm. It arises from the coracoid process of the scapula, stretches across in front of the shoulder joint and is inserted into the middle third of the humerus. It flexes the shoulder joint.
Biceps
This lies on the anterior aspect of the upper arm. At its proximal end it is divided into two parts (heads), each of which has its own tendon. The short head rises from the coracoid process of the scapula and passes in front of the shoulder joint to the arm. The long head originates from the rim of the glenoid cavity and its tendon passes through the joint cavity and the bicipital groove of the humerus to the arm. It is retained in the bicipital groove by a transverse humeral ligament that stretches across the groove. The distal tendon crosses the elbow joint and is inserted into the radial tuberosity. It helps to stabilise and flex the shoulder joint and at the elbow joint it assists with flexion and supination.
Brachialis
This lies on the anterior aspect of the upper arm deep to the biceps. It originates from the shaft of the humerus, extends across the elbow joint and is inserted into the ulna just distal to the joint capsule. It is the main flexor of the elbow joint.
Triceps
This lies on the posterior aspect of the humerus. It arises from three heads, one from the scapula and two from the posterior surface of the humerus. The insertion is by a common tendon to the olecranon process of the ulna. It helps to stabilise the shoulder joint, assists in adduction of the arm and extends the elbow joint.
Brachioradialis
The brachioradialis spans the elbow joint, originating on the distal end of the humerus and inserts on the lateral epicondyle of the radius. When it contracts, it flexes the elbow joint.
Pronator quadratus
This square-shaped muscle is the main muscle causing pronation of the hand and has attachments on the lower sections of both the radius and the ulna.
Pronator teres
This lies obliquely across the upper third of the front of the forearm. It arises from the medial epicondyle of the humerus and the coronoid process of the ulna and passes obliquely across the forearm to be inserted into the lateral surface of the shaft of the radius. It rotates the radioulnar joints, changing the hand from the anatomical to the writing position, i.e. pronation.
Supinator
This lies obliquely across the posterior and lateral aspects of the forearm. Its fibres arise from the lateral epicondyle of the humerus and the upper part of the ulna and are inserted into the lateral surface of the upper third of the radius. It rotates the radioulnar joints, often with help from the biceps, changing the hand from the writing to the anatomical position, i.e. supination. It lies deep to the muscles shown in
Figure 16.65
.
Flexor carpi radialis
This lies on the anterior surface of the forearm. It originates from the medial epicondyle of the humerus and is inserted into the second and third metacarpal bones. It flexes the wrist joint, and when acting with the extensor carpi radialis, abducts the joint.
Flexor carpi ulnaris
This lies on the medial aspect of the forearm. It originates from the medial epicondyle of the humerus and the upper parts of the ulna and is inserted into the pisiform, the hamate and the fifth metacarpal bones. It flexes the wrist, and when acting with the extensor carpi ulnaris, adducts the joint.
Extensor carpi radialis longus and brevis
These lie on the posterior aspect of the forearm. The fibres originate from the lateral epicondyle of the humerus and are inserted by a long tendon into the second and third metacarpal bones. They extend and abduct the wrist.
Extensor carpi ulnaris
This lies on the posterior surface of the forearm. It originates from the lateral epicondyle of the humerus and is inserted into the fifth metacarpal bone. It extends and adducts the wrist.
Palmaris longus
This muscle resists shearing forces that might pull the skin and fascia of the palm away from the underlying structures, and flexes the wrist. Its origin is on the medial epicondyle of the humerus, and it inserts on tendons on the palm of the hand.
Extensor digitorum
This muscle originates on the lateral epicondyle of the humerus and spans both the elbow and wrist joints; in the wrist, it divides into four tendons, one for each finger. Action of this muscle can extend any of the joints across which it passes, i.e. the elbow, wrist or finger joints.
Muscles that control finger movements
Large muscles in the forearm that extend to the hand give power to the hand and fingers, but not the delicacy of movement needed for fine and dextrous finger control. Smaller muscles, which originate on the carpal and metacarpal bones, control tiny and precise finger movements via tendinous attachments on the phalanges; muscle fibres do not extend into the fingers.
Muscles of the hip and lower limb (
Fig. 16.66
)
The biggest muscles of the body are found here, since their function is largely in weight bearing. The lower parts of the body are designed to transmit the force of body weight in walking, running, etc., evenly throughout weight-bearing structures, and as shock absorbers.
Psoas
This arises from the transverse processes and bodies of the lumbar vertebrae. It passes across the flat part of the ilium and behind the inguinal ligament to be inserted into the femur. Together with the iliacus it flexes the hip joint (see
Fig. 16.60
).
Iliacus
This lies in the iliac fossa of the innominate bone. It originates from the iliac crest, passes over the iliac fossa and joins the tendon of the psoas muscle to be inserted into the lesser trochanter of the femur. The combined action of the iliacus and psoas flexes the hip joint.
Quadriceps femoris
This is a group of four muscles lying on the front and sides of the thigh. They are the
rectus femoris
and three
vasti
: lateralis, medialis and intermedius (this last muscle is not shown in
Fig. 16.66
because it lies deep to the other two). The rectus femoris originates from the ilium and the three vasti from the upper end of the femur. Together they pass over the front of the knee joint to be inserted into the tibia by the patellar tendon. Only the rectus femoris flexes the hip joint. Together, the group acts as a very strong extensor of the knee joint.
Obturators
The obturators, deep muscles of the buttock, have their origins in the rim of the obturator foramen of the pelvis and insert into the proximal femur. Their main function lies in lateral rotation at the hip joint.
Gluteals
These consist of the
gluteus maximus
,
medius
and
minimus
, which together form the fleshy part of the buttock. They originate from the ilium and sacrum and are inserted into the femur. They cause extension, abduction and medial rotation at the hip joint.
Sartorius
This is the longest muscle in the body and crosses both the hip and knee joints. It originates from the anterior superior iliac spine and passes obliquely across the hip joint, thigh and knee joint to be inserted into the medial surface of the upper part of the tibia. It is associated with flexion and abduction at the hip joint and flexion at the knee.
Adductor group
This lies on the medial aspect of the thigh. They originate from the pubic bone and are inserted into the linea aspera of the femur. They adduct and medially rotate the thigh.
Hamstrings
These lie on the posterior aspect of the thigh. They originate from the ischium and are inserted into the upper end of the tibia. They are the
biceps femoris
,
semimembranosus
and
semitendinosus muscles
. They flex the knee joint.
Gastrocnemius
This forms the bulk of the calf of the leg. It arises by two heads, one from each condyle of the femur, and passes down behind the tibia to be inserted into the calcaneus by the
calcanean tendon
(
Achilles tendon
). It crosses both knee and ankle joints, causing flexion at the knee and plantarflexion (rising onto the ball of the foot) at the ankle.