Pocket Medicine: The Massachusetts General Hospital Handbook of Internal Medicine (122 page)
Read Pocket Medicine: The Massachusetts General Hospital Handbook of Internal Medicine Online
Authors: Marc Sabatine
Tags: #Medical, #Internal Medicine

OPHTHALMIC ISSUES
ACUTE VISUAL CHANGES
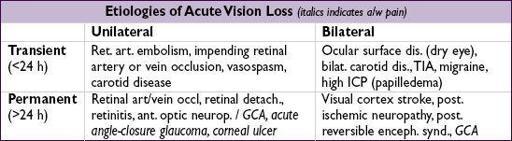
Description & common etiologies of other visual changes
•
Fluctuation in vision (ie, blurry)
: med-induced refractive error (eg, systemic steroids, chemotherapy), hyperglycemia, dry eye (common) •
Double vision (diplopia)
: fixed double vision w/ ophthalmoplegia from orbital process or cranial nerve palsy. Transient “diplopia” due to fatigue or sedation.
•
Visual field defect
: bilateral (homonymous → contral. CNS lesion; bitemporal → pituitary, glaucoma or toxic/nutritional); unilateral (ipsilat. orbital, retinal or optic nerve prob) •
Floaters
: vitreous detachment (common, benign); retinal detachment (uncommon, “flashing lights,” unilateral visual field defect); hemorrhage; intraocular lymphoma
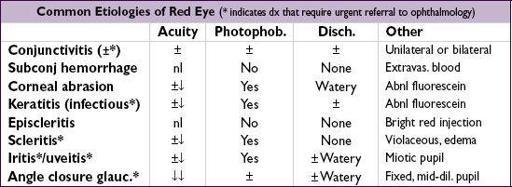
RED EYE
OTHER DIAGNOSES
Optic nerve disorders
•
Ischemic optic neuropathy
: p/w acute unilat. visual loss, altitudinal field defect
anterior
: a/w GCA; non-arteritic a/w HTN, hyperchol., DM, thrombophilia
posterior
(very rare): seen after severe blood loss; hypotension during surgery •
Optic neuritis
: often p/w unilat. central scotoma, pain with EOM,↑ visual loss over days; a/w demyelinating disease (eg, MS), also seen w/ sarcoidosis & CTD
Ocular motor palsies
•
CN III palsy:
EOM restricted in all directions except laterally (eye is “down & out”); a/w ptosis & mydriasis; seen w/ uncal herniation, aneurysm of post com art., GCA, HTN, DM
•
CN IV palsy:
upward deviation & lack of depression on adduction; congenital 4th (no diplopia); a/w trauma, post fossa tumor (vertical diplopia, better with head tilt) •
CN VI palsy:
failure of abduction (eye is “turned in”), horizontal diplopia worse at distance than near, worse w/ gaze to affected side; a/w ↑ ICP, HTN, diabetes, trauma
Other Dx
•
Orbital cellulitis
: p/w fever, proptosis, ↓ EOM, sinusitis; requires
emergent abx & referral to ophtho
; differentiate from preseptal cellulitis by presence of pain w/ eye movement, proptosis, pupil reaction abnl, ophthalmoplegia, ± visual changes •
SJS/TEN
/
facial burn/acute GVHD
: conjunctival/lid/cornea involvement → may lead to corneal perforation, permanent vision loss;
emerg ophtho consult
INITIAL EVALUATION
• Ocular presentation: onset (sudden or progressive) & duration of sx; unilateral vs. bilateral; pain; photophobia; discharge; Δ in near (eg, book) or far (eg, TV across room) vision • Pre-existing ocular conditions, eye meds (incl any Ds), recent h/o ocular surgery • Ocular exam: vision (✓with Pt’s correction [glasses/contacts]) w/ each eye; pupillary exam; EOM; confrontation visual fields (important if suspect CNS problem) • Overall status: VS, immunocompromised, s/s of infxn, h/o malignancy, CNS issues, Δ in meds, CBC, coags
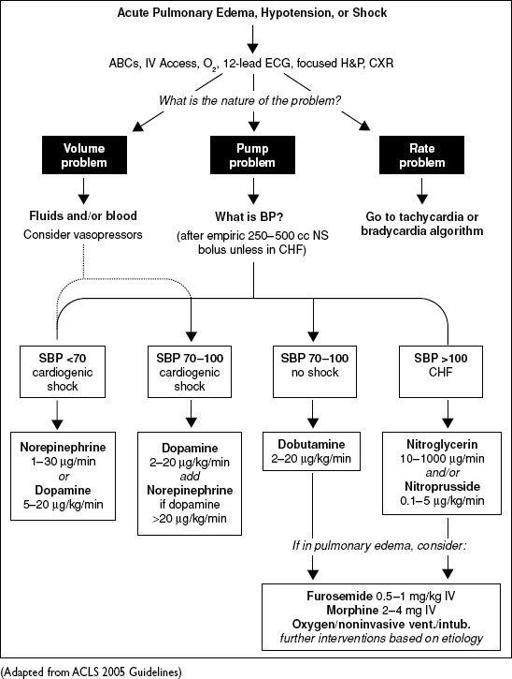
ICU MEDICATIONS
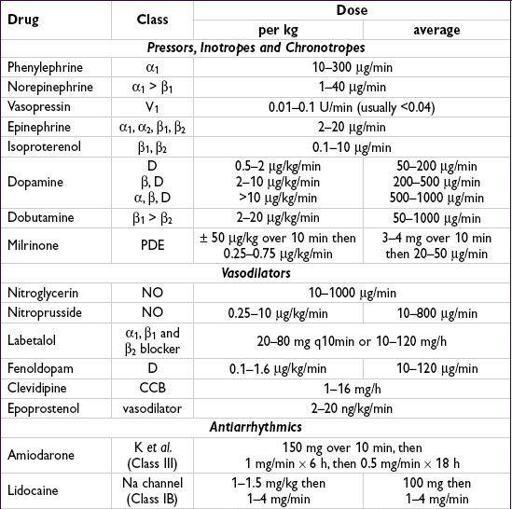
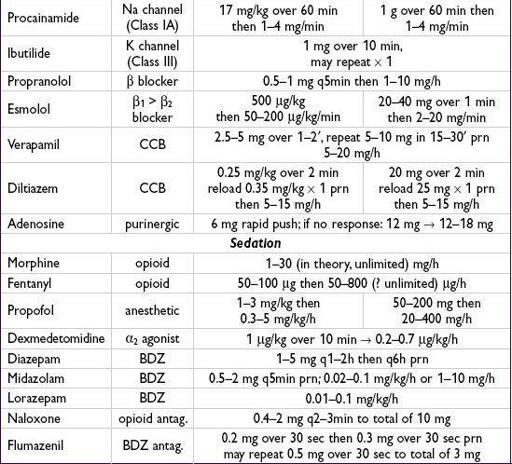
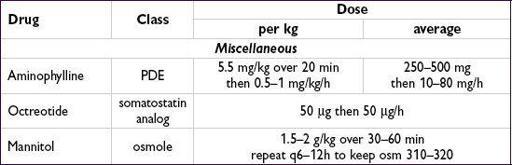
Figure 11-1 ACLS pulmonary edema, hypotension or shock algorithm
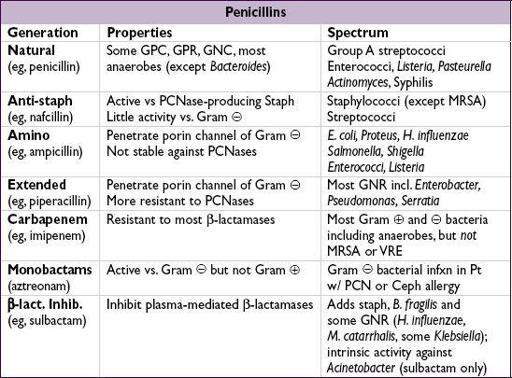
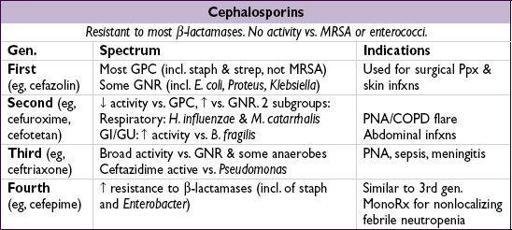
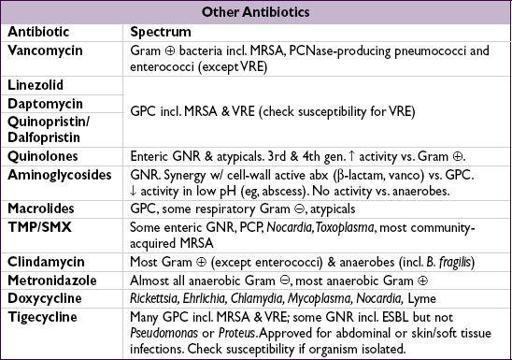
ANTIBIOTICS
The following tables of spectra of activity for different antibiotics are generalizations
.
Sensitivity data at your own institution should be used to guide therapy
.
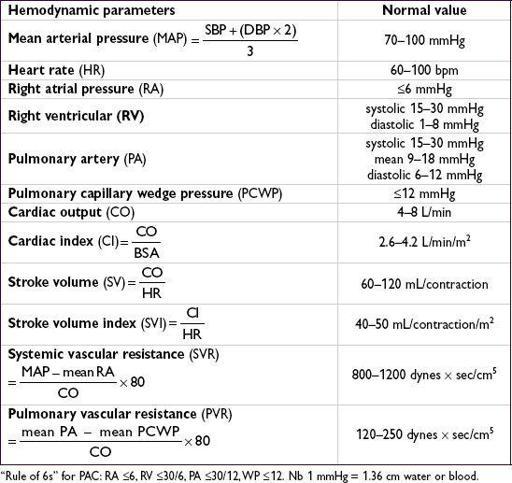
FORMULAE AND QUICK REFERENCE
CARDIOLOGY
Fick cardiac output
Oxygen consumption (L/min) = CO (L/min) × arteriovenous (AV) oxygen difference
CO = oxygen consumption/AV oxygen difference
Oxygen consumption must be measured (can estimate w/ 125 mL/min/m
2
, but inaccurate)
AV oxygen difference = Hb (g/dL) × 10 (dL/L) × 1.36 (mL O
2
/g of Hb) × (S
a
O
2
—S
v
O
2
)