Pediatric Examination and Board Review (239 page)
Read Pediatric Examination and Board Review Online
Authors: Robert Daum,Jason Canel

(A) selective dorsal rhizotomy
(B) botulinum toxin injections
(C) physical therapy
(D) baclofen
(E) all of the above
11.
A 7-year-old boy presents to your clinic for an evaluation of behavioral problems and new-onset seizures. During the last 3 months, he has received poor grades, especially in writing. His mother states that until recently he was a completely normal child. She is concerned because her estranged sister had a male child with similar symptoms before he died. In the next couple of months, the patient rapidly deteriorates. He now has a spastic paraparesis and visual loss. The study most likely to help make the diagnosis is which of the following?
(A) EEG
(B) galactocerebroside beta-galactosidase levels
(C) MRI of the brain
(D) plasma very long chain fatty acids
(E) C and D
12.
An MRI of the brain demonstrates bilateral parietooccipital white matter lesions. The most likely diagnosis in this patient is which of the following?
(A) Alexander disease
(B) X-linked adrenoleukodystrophy
(C) metachromatic leukodystrophy
(D) Canavan disease
(E) Pelizaeus-Merzbacher disease
13.
All of the following are considered lipidoses except
(A) Niemann-Pick disease
(B) Krabbe disease
(C) Tay-Sachs disease
(D) X-linked adrenoleukodystrophy
(E) Gaucher disease
14.
Which of the following statements is true regarding the genetics of Niemann-Pick disease?
(A) it is transmitted as an autosomal recessive trait
(B) it is transmitted as an autosomal dominant trait
(C) the disorder has an X-linked mode of inheritance
(D) the disorder is the result of triplet repeat expansion
(E) the disorder is the result of mutations of mitochondrial DNA
MATCH EACH OF THE FOLLOWING DISEASES WITH ITS CORRESPONDING DEFECT OR DEFICIENCY
15. | (A) beta-glucocerebrosidase |
16. | (B) methyl-CpG-binding protein (MECP) |
17. | (C) galactocerebroside beta-galactosidase |
18. | (D) arylsulfatase A |
19. | (E) hexosaminidase A |
ANSWERS
1.
(C)
IVHs occur within the germinal matrix, which, along with the germinal ventricular zone, is the site of neuronal and glial precursor cell proliferation. This structure remains relatively intact until approximately 34 weeks’ gestational age, after which it starts to involute, a process completed by term. Preterm infants are most likely to experience IVHs within the first 3-4 days following birth.
2.
(B)
There are 4 grades of IVH. A grade 1 IVH consists of bleeding within the germinal matrix. In a grade 2 IVH, blood is found within the ventricular system and there is no associated distension. If there is bleeding within the ventricle with concomitant distension, the IVH is considered grade 3. In a grade 4 IVH, there is parenchymal involvement by the hemorrhage.
3.
(B)
This case is an example of a nonprogressive encephalopathy. This child most likely has the spastic hemiplegic form of cerebral palsy given that the right side of his body is weak and spastic with increased reflexes (signs of upper motor neuron involvement). Cerebral palsy is a nonspecific term that describes a disability of motor function seen in early infancy. The patients usually have problems with muscle tone (typically spasticity), ataxia, or involuntary movements. Although cognitive, behavioral, and sensory problems can be observed in children with cerebral palsy, these features are not necessary to make the diagnosis. Patients with spastic hemiplegia can have difficulties with gross and fine motor coordination. The child is usually unable to perform a pincer grasp with the affected hand, as was the case with this child. Facial involvement is unusual in the spastic hemiplegic form of cerebral palsy. Over time the affected limbs usually undergo growth retardation. This is often best demonstrated by comparing the affected limb with the opposite normal limb. This needs to be monitored closely because a growth discrepancy of the leg may cause problems with ambulation and lead to further orthopedic difficulties. An older study looking at patients with spastic hemiplegia suggested that up to a third might have mental retardation and/or seizures. A wide range of medical conditions may lead to the spastic hemiplegic form of cerebral palsy including infarction and hemorrhage.
4.
(E)
Low birthweight and preterm delivery are significant risk factors for the development of cerebral palsy. Twin gestation also may predispose to cerebral palsy because the infants are at risk for low birthweight. Marked hyperbilirubinemia was once a common cause of choreoathetotic cerebral palsy in the setting of kernicterus. Finally, ingestion of certain toxins, such as methyl mercury, during pregnancy is associated with the subsequent development of cerebral palsy. Intrauterine and neonatal infections can also lead to the development of cerebral palsy. It should be noted that although birth trauma and asphyxia can result in cerebral palsy, they are not the leading causes.
5.
(E)
Cerebral palsy is classified according to certain neurologic signs and symptoms. These include the following: spastic, choreoathetotic, dystonic, ballismic, ataxic, and mixed. Based on the limb involvement, the classes can be further subdivided. Hence a patient with spasticity and bilateral lower extremity involvement would have spastic diplegia, whereas an individual with 4-extremity involvement would have spastic quadriplegia.
6.
(D)
This patient presents with the classical clinical tetrad observed in kernicterus: sensorineural hearing loss, supernuclear ophthalmoplegia, enamel hypoplasia, and choreoathetosis. However, rarely does one observe all 4 symptoms in a single affected patient. Kernicterus is caused by the deposition of bile pigments in various nuclei of the brain (brainstem, cerebellum, and basal ganglia) and spinal cord. Infants with marked hyperbilirubinemia may manifest symptoms as early as the second or third day of life. Sensorineural hearing loss is common and results from degeneration of the cochlear nuclei.
7.
(A)
Approximately 80% of preterm infants with the spastic form of cerebral palsy have the diplegic form. These patients have periventricular leukomalacia at the germinal matrix. Porencephalic cysts may also be observed.
8.
(C)
As stated above, facial involvement is rare in patients with spastic hemiplegia. Approximately two-thirds of patients have left hemispheric involvement for unclear reasons. The arm is usually more affected than the leg. Most children with spastic hemiplegia walk by the age of 2 years compared with spastic diplegia where a little more than half walk by 3 years of age. Spastic hemiplegic patients who learn to walk may have a circumductive gait.
9.
(B)
Birth asphyxia typically leads to the spastic quadriplegic form of cerebral palsy. In this form of cerebral palsy the legs are more involved than the arms. Approximately half of the children with spastic quadriplegia have seizures of the generalized tonic-clonic type.
10.
(E)
A major goal in the treatment of cerebral palsy is to maximize function so the patient will be able to satisfy daily needs. To that extent, all of the interventions listed in this question have been used in the treatment of cerebral palsy. Because every patient’s needs are different, the treatment is tailored to the individual patient. Physical and occupational therapy programs are almost always employed in the overall treatment plan of cerebral palsy. These therapies help increase range of motion and prevent contractures. In addition, patients are taught normal movement patterns and methods of compensation. Orthotic devices, such as braces, are employed to prevent contractures. Surgical techniques, such as selective dorsal rhizotomy, which involves cutting half of the dorsal roots, can be employed with the goal of decreasing muscle tone in the affected limb. A number of medications have been tried to reduce hypertonicity. These medications include diazepam, baclofen, and dantrolene. Baclofen can be given orally or intrathecally via an infusion pump. These medications are especially useful if the spasticity is generalized. Botulinum toxin injections offer the advantage of isolating specific muscles. The toxin inhibits the release of acetylcholine from the presynaptic terminal. The benefits of the injection typically last around 3 months.
11.
(E)
Based on the clinical history, this child has a progressive neurologic disorder as evident by the regression of skills and rapid clinical deterioration. Although the EEG would be helpful in confirming the clinical suspicion of seizures and in fact may help classify the seizure type, it is unlikely in this case to yield the diagnosis. An MRI of the brain would be helpful given the rapid development of spastic paraparesis and clinical seizures. The MRI would be able to determine whether the underlying disease process affects primarily gray matter, as would be suspected given the history of seizures, white matter, or both. A primarily white matter process would suggest a leukodystrophy; gray and white matter lesions would be suggestive of a mitochondrial process. Two disorders, globoid cell leukodystrophy (Krabbe disease) and X-linked adrenoleukodystrophy, can present with visual loss. Given the possibility that the mother’s nephew died of the same condition, an X-linked disorder should be suspected. In the early stages, involvement of the parieto-occipital white matter is seen in Krabbe disease, possibly resembling X-linked adrenoleukodystrophy. Because the latter is a peroxisomal disorder, plasma very long chain fatty acids will be increased.
12.
(B)
Given the clinical history and MRI findings, this patient most likely has X-linked adrenoleukodystrophy (see
Figure 138-1
). Male children are usually normal until 4-8 years of age when symptoms begin. This disorder is rapidly progressive. In approximately 85% of the cases, the MRI of the brain demonstrates hyperintensity of the parietooccipital white matter. Alexander and Canavan disease are 2 leukodystrophies associated with macrocephaly. Alexander disease has a predilection for the frontal white matter, whereas the MRI findings in Canavan disease show diffuse white matter involvement with prominent involvement of the subcortical U fibers. The MRI of a patient with Pelizaeus-Merzbacher disease demonstrates heterogeneous hyperintense lesions in the white matter with scattered small foci of normal areas, lending the name “tigroid” pattern .
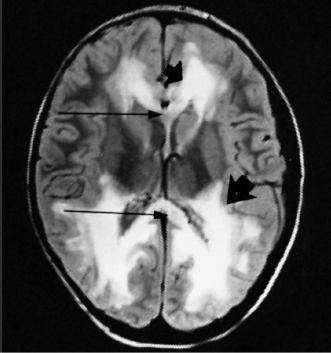
FIGURE 138-1
.
Adrenal leukodystrophy in a 7-year-old male. Confluent areas of increased signal involving the frontal, occipital, and parietal white matter (thick arrows) and of the anterior and posterior portions of the corpus callosum (long stemmed arrows). (Reproduced, with permission, from Bisese JH. Cranial MRI. New York: McGraw-Hill; 1991.)
13.
(D)
The term
lipidoses
refers to a group of inherited disorders in which lipid metabolism is abnormal. Lysosomal enzymes are affected. Niemann-Pick disease (sphingomyelin lipidosis), Krabbe disease (galactosylceramide lipidosis), Tay-Sachs disease (GM
2
gangliosidosis), and Gaucher disease (glucosylceramide lipidosis) are all examples of lipidoses. X-linked adrenoleukodystrophy is an example of a peroxisomal disorder.