Pocket Medicine: The Massachusetts General Hospital Handbook of Internal Medicine (7 page)
Read Pocket Medicine: The Massachusetts General Hospital Handbook of Internal Medicine Online
Authors: Marc Sabatine
Tags: #Medical, #Internal Medicine

BOOK: Pocket Medicine: The Massachusetts General Hospital Handbook of Internal Medicine
12.65Mb size Format: txt, pdf, ePub
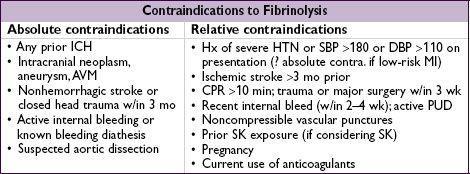
Fibrinolysis
• Indic: STE/LBBB + sx <12 h; benefit if sx >12 h less clear; reasonable if persist. sx & STE
• Mortality ↓
20% in anterior MI or LBBB and
10% in IMI c/w reperfusion Rx • Prehospital lysis (ie, ambulance): further 17% ↓ in mortality (
JAMA
2000;283:2686) •
1% risk of ICH; high-risk groups include elderly (
2% if >75 y), women, low wt • Although age not contraindic., ↑ risk of ICH in elderly (>75 y) makes PCI more attractive
Nonprimary PCI
• Facilitated PCI: upstream lytic, GPI or GPI + ½ dose lytic before PCI offers no benefit • Rescue PCI if shock, unstable, failed reperfusion or persistent sx (
NEJM
2005;353:2758) • Routine angio ± PCI w/in 24 h of successful lysis: ↓ D/MI/revasc (
Lancet
2004;364:1045) and w/in 6 h ↓ reMI, recurrent ischemia, & HF compared to w/in 2 wk (
NEJM
2009;360:2705);
∴
if lysed at non-PCI capable hospital, consider transfer to PCI-capable hospital ASAP esp. if high-risk presentation (eg, anterior MI, inferior MI w/ low EF or RV infarct, extensive STE or LBBB, HF
, ↓
BP or
↑
HR
)
•
Late
PCI (median day 8) of occluded infarct-related artery: no benefit (
NEJM
2006;355:2395)
LV failure (~25%)
• Diurese to achieve PCWP 15–20 → ↓ pulmonary edema, ↓ myocardial O
2
demand • ↓ Afterload → ↑ stroke volume & CO, ↓ myocardial O
2
demand
can use IV NTG or nitroprusside (risk of coronary steal) → short-acting ACEI
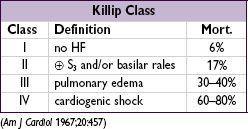
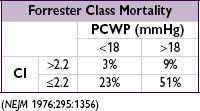
• Inotropes if HF despite diuresis & ↓ afterload; use dopamine, dobutamine or milrinone •
Cardiogenic shock
(~7%) = MAP <60 mmHg, CI <2 L/min/m
2
, PCWP >18 mmHg; inotropes, mech support [eg, VAD, IABP (trial w/o benefit
NEJM
2012;367:1287)] to keep CI >2; pressors to keep MAP >60; if not done already, coronary revasc (
NEJM
1999;341:625)
IMI complications (
Circ
1990;81:401;
NEJM
1994;330:1211;
JACC
2003;41:1273)
•
Heart block
(~20%, occurs because RCA typically supplies AV node)
40% on present., 20% w/in 24 h, rest by 72 h; high-grade AVB can develop abruptly
Rx: atropine, epi, aminophylline (100 mg/min × 2.5 min), temp wire
•
RV infarct
(30–50%, but only ½ of those clinically signif). HoTN; ↑ JVP,Kussmaul’s; 1 mm STE in V
4
R; RA/PCWP ≥0.8; RV dysfxn on TTE; prox RCA occl.
Rx: optimize preload (RA goal 10–14,
BHJ
1990;63:98); ↑ contractility (dobutamine); maintain AV synchrony (pacing as necessary); reperfusion (
NEJM
1998;338:933); mechanical support (IABP or RVAD); pulmonary vasodilators (eg, inhaled NO)
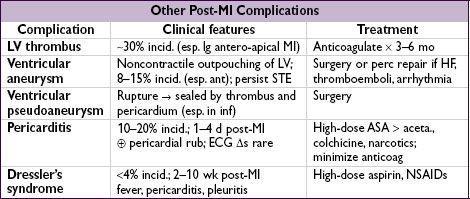
Mechanical complications (incid. <1% for each; typically occur a few days post-MI)
•
Free wall rupture
: ↑ risk w/ lysis, large MI, ↑ age,, HTN; p/w PEA or hypoTN, pericardial sx, tamponade; Rx: volume resusc., ? pericardiocentesis, inotropes,
surgery
•
VSD
: large MI in elderly; AMI → apical VSD, IMI → basal septum; 90% w/ harsh murmur ±
thrill (
NEJM
2002;347:1426); Rx: diuretics, vasodil., inotropes, IABP,
surgery
, perc. closure
•
Papillary muscle rupture
: more common after inf MI (PM pap. muscle supplied by PDA alone) than ant MI (AL pap. muscle supplied by diags & OMs); 50% w/ new murmur, rarely a thrill, ↑
v
wave in PCWP tracing; asymmetric pulmonary edema. Rx: diuretics, vasodilators, IABP,
surgery
.
Arrhythmias post-MI
• Treat as per ACLS for unstable or symptomatic bradycardias & tachycardias •
AF
(10–16% incidence): β-blocker or amio, ± digoxin (particularly if HF), heparin •
VT/VF
: lido or amio × 6–24 h, then reassess; ↑ βB as tol., replete K & Mg, r/o ischemia;
early monomorphic (<48 h post-MI) does
not
carry bad prognosis
• Accelerated idioventricular rhythm (AIVR): slow VT (<100 bpm), often seen after
successful reperfusion; typically self-terminates and does not require treatment
• May consider
backup
transcutaneous pacing
(TP) if: 2° AVB type I, BBB
•
Backup TP
or
initiate transvenous pacing
if: 2° AVB type II; BBB + AVB
•
Transvenous pacing
(TV) if: 3° AVB; new BBB + 2° AVB type II; alternating LBBB/RBBB (can bridge w/ TP until TV, which is best accomplished under fluoroscopic guidance)
Prognosis
• In registries, in-hospital mortality is 6% w/ reperfusion Rx (lytic or PCI) and ~20% w/o • Predictors of mortality: age, time to Rx, anterior MI or LBBB, heart failure (
Circ
2000;102:2031)
Other books
Benny: A Tale of a Christmas Toy by K. C. Scott
Beauty and the Biker by Riley, Alexa
I Too Had a Love Story by Ravinder Singh
On His Terms by Sierra Cartwright
Scar Night by Alan Campbell
Brides of Iowa by Stevens, Connie;
Yok by Tim Davys
Life After Life by Kate Atkinson
Surrender by Elana Johnson