Pocket Medicine: The Massachusetts General Hospital Handbook of Internal Medicine (45 page)
Read Pocket Medicine: The Massachusetts General Hospital Handbook of Internal Medicine Online
Authors: Marc Sabatine
Tags: #Medical, #Internal Medicine

BOOK: Pocket Medicine: The Massachusetts General Hospital Handbook of Internal Medicine
6.72Mb size Format: txt, pdf, ePub
Hepatitis B
(dsDNA; ~45% of acute viral hepatitis in U.S.;
Lancet
2009;373:582)
• Transmission: blood (IVDU, transfusion), sexual, perinatal
• Incubation: 6 wk–6 mo (mean 12–14 wk)
• Acute infxn: 70% subclinical, 30% jaundice, <1% fulminant hepatitis (up to 60% mortality) • Chronic infxn: <5% (adult-acquired; higher if immunosupp), >90% (perinatally acquired); ~40% chronic carriers → cirrhosis; ↑ risk of cirrhosis if HCV, HDV or HIV coinfection • Hepatocellular carcinoma (w/ or w/o concurrent cirrhosis); ↑ risk w/ perinatal transmission & ↑’d HBV DNA. Screen chronic carriers w/ AFP & U/S vs. MRI q6mo.
• Extrahepatic syndromes: PAN (<1%), MPGN, arthritis, dermatitis, PMR
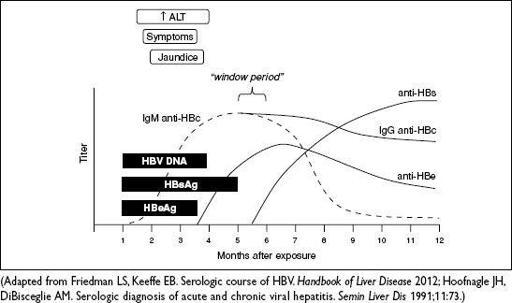
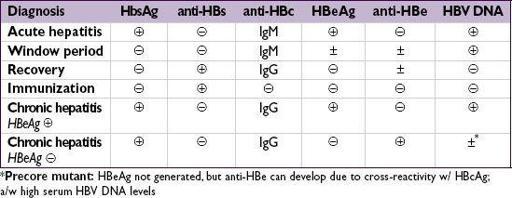
• Serologic and virologic tests
HBsAg: appears before sx; used to screen blood donors; persists >6 mo = chronic HBV
HBeAg: evidence of viral replication and ↑ infectivity
IgM anti-HBc: first Ab to appear; indicates acute infection window period = HBsAg become, anti-HBs not yet
, anti-HBc only clue to infection
IgG anti-HBc: indicates previous (HBsAg
anti-HBe: indicates waning viral replication, ↓ infectivity
anti-HBs: indicates resolution of acute disease & immunity (sole marker after vac)
HBV DNA: presence in serum correlates w/ active viral replication in liver
Figure 3-7
Serologic course of acute HBV infection with resolution
• Treatment for acute HBV: supportive; hospitalize for Δ MS or ↑ INR (liver transplant ctr) • Treatment for chronic HBV if: (1) HBeAg
NEJM
2008;359:1486;
Hep
2009;50:661;
Clin Gas Hep
2011;9:285) • 1st line is nucleo(s/t)ide analogues:
entecavir
or
tenofovir
; well tolerated & low resistance (1% for entecavir at 5 y in Rx-naïve Pts); at 5 y HBeAg seroconversion is 30–40% & loss of HBsAg is 5–10% (
Gastro
2012;142:1360;
Lancet
2013;381:468) •
PEG IFN
ɑ-2a: best rate of HBeAg seroconversion at 1 y (27%), low tolerability limits use • Goal: if HBeAg
coinfection
: Rx w/ 2 drugs active against both HBV & HIV (
NEJM
2007;356:1445) • If inactive carrier scheduled to receive immunosuppression/chemotherapy → Rx
Other books
Small-Town Cinderella (The Pirelli Brothers) by Stacy Connelly
The Jealous Kind by James Lee Burke
Jack & Diane by Hampton, Lena
1958 - The World in My Pocket by James Hadley Chase
Skylight Confessions by Alice Hoffman
In the Clear by Anne Carter
Marion Zimmer Bradley's Ancestors of Avalon by Diana L. Paxson
Eastshore Tigers 01 - Strong Side by Alison Hendricks
Hardy 05 - Mercy Rule, The by John Lescroart