Pocket Medicine: The Massachusetts General Hospital Handbook of Internal Medicine (16 page)
Read Pocket Medicine: The Massachusetts General Hospital Handbook of Internal Medicine Online
Authors: Marc Sabatine
Tags: #Medical, #Internal Medicine

BOOK: Pocket Medicine: The Massachusetts General Hospital Handbook of Internal Medicine
11.85Mb size Format: txt, pdf, ePub
PERICARDIAL DISEASE
GENERAL PRINCIPLES
Anatomy
• 2-layered (parietal & visceral) tissue sac surrounding heart & proximal great vessels
Disease states
• Inflammation (w/ or w/o fluid accumulation) → pericarditis
• Fluid accumulation → effusion ± tamponade
• Decrease in compliance (sequela of inflammation) → constrictive pericarditis
• Tamponade and constriction characterized by increased ventricular interdependence
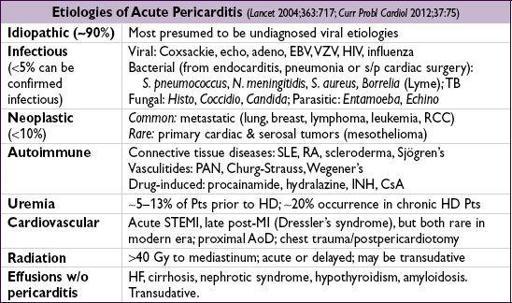
PERICARDITIS AND PERICARDIAL EFFUSION
Clinical manifestations (
NEJM
2004;351:2195)
•
Pericarditis
: retrosternal chest pain that is pleuritic, positional (↓ by sitting forward), radiates to trapezius; may be
absent
in tuberculous, neoplastic, post-XRT and uremic pericarditis; ± fever; ± s/s of systemic etiologies •
Effusion
: ranges from asx to tamponade (see below)
Physical exam
•
Pericarditis
: multiphasic
friction rub
best heard at LLSB w/ diaphragm of stethoscope. Notoriously variable and evanescent leathery sound w/ up to 3 components: atrial contraction, ventricular contraction, ventricular relaxation (
NEJM
2012;367:e20).
•
Effusion
: distant heart sounds, dullness over left posterior lung field due to compressive atelectasis from pericardial effusion (Ewart’s sign)
Diagnostic studies (
EHJ
2004;25:587;
Circ
2006;113:1622 & 2010;121:916)
• ECG: may show diffuse STE (
concave up
) & PR depression (except in aVR: ST ↓ & PR ↑), TWI; classically and in contrast to STEMI, TWI do not occur until STs normalize
Stages: (I) STE & PR ↓; (II) ST & PR normalize; (III) diffuse TWI; (IV) Tw normalize
ECG may show evidence of large effusion w/ low voltage & electrical alternans (beat-to- beat Δ in QRS amplitude and/or axis due to swinging heart)
• CXR: if large effusion (>250 mL of fluid) → ↑ cardiac silhouette w/ “water-bottle” heart and epicardial halo •
Echocardiogram
: presence, size, & location of
effusion
; presence of
tamponade physiology
; pericarditis itself w/o spec. abnl (∴ echo can be nl), although can see pericardial stranding (fibrin or tumor); can also detect LV/RV dysfxn (myocarditis ?) • CT will reveal pericardial effusions, often appearing larger than on echocardiography • CK-MB or troponin (in ~30%,
JACC
2003;42:2144) if myopericarditis. Consider CRP/ESR.
Workup for effusion
• r/o infxn: usually apparent from Hx & CXR; ? value of ✓ acute and convalescent serologies • r/o noninfectious etiologies: BUN, Cr, ANA, RF, HIV, screen for common malignancies • Pericardiocentesis if suspect infxn or malignancy or large effusion (>2 cm) or recurrent
✓ cell counts, TP, LDH, glc, Gram stain & Cx, AFB, cytology
ADA, PCR for MTb, and specific tumor markers as indicated by clinical suspicion
“exudate” criteria: TP >3 g/dL, TP
eff
/TP
serum
>0.5, LDH
eff
/LDH
serum
>0.6 or glc <60 mg/dL high Se (~90%) but
very low
Sp (~20%); overall low utility (
Chest
1997;111:1213)
• Pericardial bx if suspicion remains for malignancy or tuberculosis
Treatment of pericarditis (
EHJ
2004;25:587;
Circ
2006;113:1622)
• NSAIDs (eg, ibuprofen 600–800 mg tid × 7–14 d then taper) ± colchicine 1–2 mg × 1 → 0.5–1 mg bid × 3 mo (
Circ
2005;112:2012;
Heart
2012;98:1078); sx usually subside in 1–3 d • Steroids (usually systemic; occ. intrapericardial) only for systemic rheum or autoimmune disorder, uremic, preg., contraindication to NSAID, or refractory idiopathic dis.
Systemic steroids appear to ↑ rate of pericarditis recurrence (
Circ
2008;118:667).
• Avoid anticoagulants • Infectious effusion → pericardial drainage (preferably surgically) + systemic antibiotics • Acute idiopathic effusion self-limited in 70–90% of cases • Recurrent pericarditis (
Circ
2007;115:2739)
risk factors: subacute, lg effusion/tamponade, T >38°C, lack of NSAID response after 7 d treatment: add colchicine 0.5–1 mg bid × 6 mo (
Annals
2011;155:409)
• Recurrent effusion: consider pericardial window (percutaneous vs. surgical)
PERICARDIAL TAMPONADE
Etiology
• Any cause of pericarditis but esp.
malignancy
,
uremia
,
idiopathic
, proximal aortic dissection with rupture, myocardial rupture • Rapidly accumulating effusions most likely to cause tamponade as no time for pericardium to stretch (eg, to ↑ compliance) and accommodate ↑ intrapericardial fluid volume
Pathophysiology (
NEJM
2003;349:684)
• ↑ intrapericardial pressure, compression of heart chambers, ↓ venous return → ↓ CO
• Diastolic pressures ↑ & equalize in all cardiac chambers → minimal flow of blood from RA to RV when TV opens → blunted
y
descent • ↑ ventricular interdependence → pulsus paradoxus (pathologic exaggeration of nl physio)
Inspiration → ↓ intrapericardial & RA pressures → ↑ venous return → ↑ RV size → septal shift to left. Also, ↑ pulmonary vascular compliance → ↓ pulm venous return. Result is ↓ LV filling → ↓
LV stroke volume
& blood pressure.
Clinical manifestations
•
Cardiogenic shock
(hypotension, fatigue)
without pulmonary edema
• Dyspnea (seen in ~85%) may be due to ↑ respiratory drive to augment venous return
Physical exam (
JAMA
2007;297:1810)
•
Beck’s triad
(present in minority of cases):
distant heart sounds
, ↑
JVP
,
hypotension
• ↑ JVP (76%) w/ blunted
y
descent • Reflex tachycardia (77%), hypotension (26%; occasionally hypertensive), cool extremities •
Pulsus paradoxus
(Se 82%, Sp 70%) = ↓ SBP ≥10 mmHg during inspiration
LR 0.03
Ddx = PE, hypovolemia, severe COPD, constriction (~
1
⁄
3
), RV infarct
Can be absent if pre-existing ↑ LVEDP, arrhythmia, severe AI, ASD, regional tamponade
• Distant heart sounds (28%), ± pericardial friction rub (30%) • Tachypnea but clear lungs
Diagnostic studies
• ECG: ↓ voltage (seen in 42%), electrical alternans (20%), ± signs of pericarditis • CXR: ↑ cardiac silhouette (89%) •
Echocardiogram
:
, IVC plethora,
septal shift
with inspiration
diastolic collapse
of RA (Se 85%, Sp 80%) and/or RV (Se <80%, Sp 90%)
respirophasic
Δ
’s in transvalvular velocities
(↑ across TV & ↓ across MV w/ inspir.)
postsurgical tamponade may be localized and not easily visible
• Cardiac cath (right heart and pericardial): elevation (15–30 mmHg) and equalization of
intrapericardial and diastolic pressures (RA, RV, PCWP), blunted
y
descent in RA
↑ in stroke volume postpericardiocentesis = ultimate proof of tamponade
Other books
Back to Life by Danielle Allen
The Realms of Animar by Black, Owen
The Sheikh's First Christmas - A Warm and Cozy Christmas Romance by Rayner, Holly
The Decaying World Saga (Book 1): Tribes of Decay by Garza, Michael W.
Escorting the Actress (The Escort Collection Book 2) by Leigh James
The Water Devil by Riley, Judith Merkle
Simon Says: Mine: A novella (Mountain Masters & Dark Haven Book 2) by Sinclair, Cherise
Wanted: Devils Point Wolves #3 (Mating Season Collection) by Gayle, Eliza, Collection, Mating Season
Trust Me by John Updike
Does it Hurt to Die by Anderson, Paul G