Pocket Medicine: The Massachusetts General Hospital Handbook of Internal Medicine (13 page)
Read Pocket Medicine: The Massachusetts General Hospital Handbook of Internal Medicine Online
Authors: Marc Sabatine
Tags: #Medical, #Internal Medicine

BOOK: Pocket Medicine: The Massachusetts General Hospital Handbook of Internal Medicine
7.27Mb size Format: txt, pdf, ePub
• Congestive hepatomegaly, ± ascites and jaundice, peripheral edema
Diagnostic studies
• CXR: normal ventricular chamber size, enlarged atria, ± pulmonary congestion • ECG: low voltage, pseudoinfarction pattern (Qw), ± arrhythmias • Echo: symmetric wall thickening, biatrial enlarge., ± mural thrombi, ± cavity oblit. w/ diast dysfxn: ↑ early diast (E) and ↓ late atrial (A) filling, ↑ E/A ratio, ↓ decel. time • Cardiac MRI/PET: may reveal inflammation or evidence of infiltration (but nonspecific) • Cardiac catheterization
Atria:
M’s
or
W’s
(prominent
x
and
y
descents)
Ventricles:
dip & plateau
(rapid ↓ pressure at onset of diastole, rapid ↑ to early plateau)
Concordance
of LV and RV pressure peaks during respiratory cycle (vs. discordance in constrictive pericarditis;
Circ
1996;93:2007)
• Endomyocardial biopsy if suspect infiltrative process • Restrictive cardiomyopathy vs. constrictive pericarditis: see “Pericardial Disease”
Treatment (in addition to Rx’ing underlying disease)
• Gentle diuresis. May not tolerate CCB or other vasodilators.
• Control HR (but can ↓ CO); maintain SR (helps filling). Digoxin ↑ arrhythmias in amyloid.
• Anticoagulation (particularly with AF or low CO) • Transplantation for refractory cases
VALVULAR HEART DISEASE
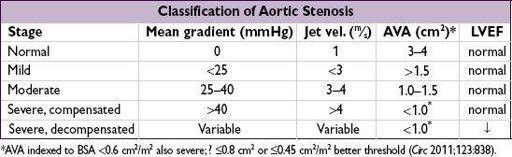
AORTIC STENOSIS (AS)
Etiology
•
Calcific
: predominant cause in Pts >70 y; risk factors include HTN, ↑ chol., ESRD
•
Congenital
(ie, bicuspid AoV w/ premature calcification): cause in 50% of Pts <70 y •
Rheumatic heart disease
(AS usually accompanied by AI and MV disease) • AS mimickers: subvalvular (HCMP, subAo membrane) or supravalvular stenosis
Clinical manifestations (usually indicates AVA <1 cm
2
or concomitant CAD)
•
Angina
: ↑ O
2
demand (hypertrophy) + ↓ O
2
supply (↓ cor perfusion pressure) ± CAD
•
Syncope
(
exertional
): peripheral vasodil. w/ fixed CO → ↓ MAP → ↓ cerebral perfusion •
Heart failure
: outflow obstruct + diastolic dysfxn → pulm. edema; esp. if ↑ HR/AF (↓ LV fill.) • Acquired vWF disease (~20% of sev. AS): destruction of vWF; GI angiodysplasia • Natural hx: usually slowly progressive (AVA ↓ ~0.1 cm
2
/y, but varies;
Circ
1997;95:2262), until sx develop; mean survival based on sx: angina = 5 y; syncope = 3 y; CHF = 2 y
Physical exam
•
Midsystolic crescendo-decrescendo
murmur at
RUSB
, harsh, high-pitched, radiates to carotids, apex (holo-systolic = Gallavardin effect), ↑ w/ passive leg raise, ↓ w/ standing & Valsalva. In contrast, dynamic outflow obstruction (HCMP) ↓ w/ leg raise, ↑ w/ standing, Valsalva.
• Ejection click after S1 sometimes heard with
bicuspid
AoV
• Signs of severity:
late-peaking
murmur, paradoxically split S
2
or inaudible A
2
, small and delayed carotid pulse (“
pulsus parvus et tardus
”), LV heave,S
4
(occasionally palpable)

Diagnostic studies
• ECG: may see LVH, LAE, LBBB, AF (in late disease) • CXR: cardiomegaly, AoV calcification, poststenotic dilation of ascending Ao, pulmonary congestion •
Echo
: valve morphology, estim pressure gradient & calculate AVA, EF
•
Cardiac cath
: usually to
r/o CAD
(in ~½ of calcific AS); for hemodyn. if disparity between exam & echo: ✓ pressure gradient (∇) across AoV, calc AVA (underestim. if mod/sev AI) •
Dobutamine challenge
during echo or cath if low EF and ∇ <30 to differentiate:
afterload mismatch:
20% ↑ SV & ∇, no Δ AVA (implies contractile reserve & ↑ EF post-AVR)
pseudostenosis:
20% ↑ SV, no Δ in ∇, ↑ AVA (implies low AVA
artifact
of LV dysfxn)
limited contractile reserve:
no Δ SV, ∇ or AVA (implies EF prob. will not improve w/ AVR)
Treatment (
Circ
2008;118:e523;
Lancet
2009;373:956;
EHJ
2012;33:2451)
• Management decisions are based on
symptoms
: once they develop AVR is needed.
If asx, HTN can be cautiously Rx’d; statins have not been proven to ↓ progression.
•
AVR
: indicated in
sx AS
(almost invariably severe; if not, look for another cause of sx) &
asx severe AS
+
EF
<
50%.
May consider if
asx
but
either sx or
↓
BP w/ exercise
(can
carefully
exercise asx AS to uncover sx, do
not
exercise sx AS) or
extremely severe
(AVA <0.6 cm
2
, mean ∇ >60 mmHg, aortic jet >5 m/s). Reasonable if asx mod-severe AS
and
undergoing CV surgery.
• Medical (if not AVR candidate or to temporize): careful diuresis prn, control HTN, maintain SR; digoxin if ↓ EF & HF or if AF;
avoid
venodilators (nitrates) &inotropes (bB/CCB) if severe; avoid vigorous physical exertion once AS mod–severe;
? nitroprusside if p/w CHF w/ sev. AS, EF <35%, CI <2.2, & nl BP (
NEJM
2003;348:1756)
• IABP: stabilization, bridge to surgery • Balloon AoV valvotomy (BAV): 50% ↑ AVA & ↓ peak ∇,
but
50% restenosis by 6–12 mo &
↑ risk of peri-PAV stroke/AI (
NEJM
1988;319:125), ∴ bridge to AVR or palliation
•
Transcatheter AoV replacement (TAVR)
:sx, hemodyn, & mortality to surgical AVR, but ↑ (mostly early) risk of vasc complic and stroke/ TIA; paravalvular leaks in ~7% (
NEJM
2012;366:1686); in nonoperative Pts, 44% ↓ mortality vs. standard Rx (
NEJM
2012;366:1696)
AORTIC INSUFFICIENCY (AI)
Etiology (
Circ
2006;114:422)
•
Valve disease
(43%)
rheumatic heart disease
(usually mixed AS/AI and concomitant MV disease)
bicuspid AoV
: natural hx:
1
⁄
3
→ normal,
1
⁄
3
→ AS,
1
⁄
6
→ AI,
1
⁄
6
→ endocarditis → AI
infective endocarditis
valvulitis: RA, SLE; anorectics (fen/phen) & other serotoninergics (
NEJM
2007;356:29,39), XRT
•
Root disease
(57%)
HTN
aortic aneurysm or dissection, annuloaortic ectasia, Marfan syndrome
aortic inflammation: giant cell, Takayasu’s, ankylosing spond., reactive arthritis, syphilis
Clinical manifestations
• Acute: sudden ↓ forward SV and ↑ LVEDP (noncompliant ventricle) → pulmonary edema ± hypotension and cardiogenic shock • Chronic: clinically silent while LV dilates (to ↑ compliance to keep LVEDP low) more than it hypertrophies → chronic volume overload → LV decompensation → CHF
• Natural hx:
variable
progression (unlike AS, can be fast or slow); once decompensation begins, prognosis poor w/o AVR (mortality ~10%/y)
Physical exam
Other books
El hombre de los círculos azules by Fred Vargas
California by Banks, Ray
Sex Slave at Sea by Aphrodite Hunt
Deliverance by T.K. Chapin
Redheart (Leland Dragon Series) by Jackie Gamber
Sisters by Danielle Steel
The Doctor's Christmas Bride by Sarah Morgan
Taming Her Heart by Marisa Chenery
In My Arms Tonight by Bailey Bradford
Secrets Of The Heart (Book 1, The Heart Series) by LeClair, Laurie