Pediatric Examination and Board Review (89 page)
Read Pediatric Examination and Board Review Online
Authors: Robert Daum,Jason Canel

(A) rapid growth
(B) dislocation of the femoral head
(C) bacterial invasion of the femoral head capsule
(D) poor blood supply to the femoral head
(E) immature bone development
3.
What is the best test to order first?
(A) CBC with differential
(B) ultrasound
(C) radiograph
(D) CT scan
(E) magnetic resonance imaging (MRI)
4.
If a radiograph of the hips is normal, what is the best course of action at this time for this 5-year-old boy?
(A) brace
(B) serial casting
(C) surgical correction
(D) observation
(E) physical therapy
5.
A 6-year-old boy is brought in for a painful limp of 2 days’ duration on the left side. He recalls no trauma to the affected leg and has only been getting mild relief with nonsteroidal anti-inflammatory compounds. His recent medical history includes a “viral illness” several weeks ago and a temperature of 100°F (37.7°C) each day. On examination you note that he holds the left hip in a flexed, externally rotated position, and he has pain on internal rotation. There is no erythema or warmth over the area. What is the most likely diagnosis?
(A) transient synovitis or septic arthritis
(B) SCFE
(C) Legg-Calvé-Perthes disease
(D) growing pains
(E) none of the above
6.
Which of the following tests would be most helpful to make a diagnosis for the patient in question 5?
(A) radiographs
(B) CBC
(C) erythrocyte sedimentation rate (ESR)
(D) synovial fluid aspirate with gram stain and culture of the fluid obtained
(E) MRI
7.
A 14-year-old boy is in your office for a sports physical examination for football and on questioning admits that he has had a limp for about 1 month that he states is a result of a “pulled muscle” that occurred during a workout session. He complains of intermittent pain in his right knee and thigh. He has been afebrile and has been able to play sports, although there is pain with activity.
On examination his BMI is 31 kg/m
2
(>95%). His musculoskeletal examination is significant for his right leg that is held in external rotation. He has pain in the right hip on internal rotation. He is able to bear weight but walks with a limp on the right. What is the most likely diagnosis?
(A) inguinal hernia
(B) SCFE
(C) Legg-Calvé-Perthes disease
(D) septic arthritis
(E) growing pains
8.
Which of the following is true of the disorder described in question 7?
(A) it has equal incidence in males and females
(B) it is more common in overweight or obese adolescents
(C) it is more common in rapidly growing adolescents
(D) it is almost always bilateral
(E) B and C
9.
What is the most appropriate way to treat the disorder described in question 7?
(A) rest and ice compresses
(B) nonsteroidal anti-inflammatory drugs (NSAIDs)
(C) surgical pinning
(D) serial casting
(E) observation
10.
In a sports physical examination performed on a 14-year-old soccer-playing boy, you are told about pain below the knee that worsens without other symptoms when he is playing soccer. On physical examination he has a hard prominence over the tibial tubercle that is tender on palpation. The rest of his examination is normal. What is your diagnosis?
(A) osteosarcoma
(B) Osgood-Schlatter disease
(C) septic arthritis
(D) patellofemoral stress syndrome
(E) stress fracture
11.
What other physical examination findings might there be in question 7?
(A) knee effusion
(B) tight quadriceps and/or hamstring muscle(s)
(C) diminished deep tendon reflexes
(D) B and C
(E) none of the above
12.
What is the best treatment for the patient’s problem in question 10?
(A) brace
(B) surgical correction
(C) rest and NSAIDs
(D) corticosteroid injection
(E) no treatment is indicated
13.
During a sports physical examination of a 10-yearold girl, you note mild lateral asymmetry of her thoracic spine on standing, and moderate to severe asymmetry of her posterior chest on forward bending. She is Tanner 2 breast, Tanner 1 pubic hair. What is the next appropriate action?
(A) observation and reexamination next year
(B) surgical consultation for back brace placement
(C) physical therapy
(D) MRI of the thoracolumbar spine
(E) posteroanterior (PA) radiographs
14.
Which of the following is associated with congenital scoliosis?
(A) horseshoe kidney
(B) hip dysplasia
(C) spinal dysraphism
(D) congenital heart disease
(E) all of the above
15.
At what age should girls begin to have scoliosis screening examinations?
(A) 2 years
(B) 5 years
(C) 7 years
(D) 12 years
(E) 15 years
16.
What is the Cobb angle cutoff whereby a patient with a greater angle is likely to develop pulmonary problems because of their scoliosis?
(A) 10 degrees
(B) 20 degrees
(C) 40 degrees
(D) 60 degrees
(E) 80 degrees
17.
Which of the following is true of most cases of kyphosis in adolescents?
(A) it is usually postural
(B) therapy is exercise to strengthen abdominal muscles
(C) kyphosis corrects with hyperextension
(D) patients have normal radiographs
(E) all of the above
18.
What distinguishes postural kyphosis from Scheuermann kyphosis in adolescents?
(A) etiology
(B) examination
(C) radiographic findings
(D) treatment
(E) all of the above
ANSWERS
1.
(C)
This is the classic presentation of Legg-Calvé-Perthes disease, a disorder of the femoral head that causes a painless limp in prepubertal, immature children, 2-12 years old (mean: 7 years old). There is a predilection for boys (4 to 5:1). It is sometimes associated with delayed bone age, disproportionate growth, and short stature, as in this case (see
Figure 55-1
).
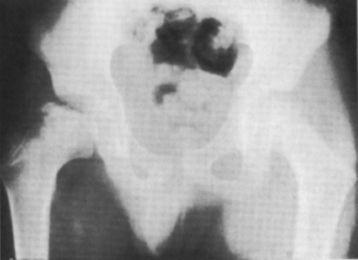
FIGURE 55-1.
X-ray of Legg Perthes disease with significant deformity of right femoral head. (Reproduced, with permission, from Doherty G. Current Diagnosis & Treatment: Surgery, 13th ed. New York: McGraw-Hill; 2010: Fig. 40-28.)
2.
(D)
A poor blood supply to the femoral head causes avascular necrosis, whose cause is unknown.
3.
(C)
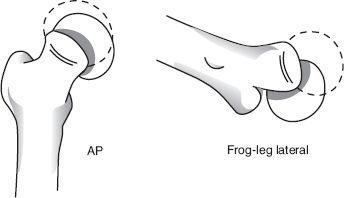
Anteroposterior (AP) and lateral (frog) views are the gold standard for diagnosis. Often the radiographs are normal, although several groups have developed diagnostic criteria that depend on the degree of growth cessation of the capital femoral epiphysis, presence of any subchondral fracture, and degree of resorption and reossification.
4.
(D)
Observation is the rule in children younger than 6 years old (possibly <5 years for girls), unless there is significant deformity of the capital femoral epiphysis on the radiographs. If pain is present, temporary physical therapy and bed rest may be in order.
5.
(A)
Transient synovitis and septic arthritis can be difficult to differentiate without further testing. Both usually present with a unilateral painful limp and often with fever. Transient synovitis is the most common cause of nontraumatic hip pain in children. It is an inflammatory process that often follows a viral illness, although no specific virus has been implicated. The painful limp can be acute or gradual in onset and is usually unilateral.
6.
(D)
A positive culture from a joint aspirate or blood are gold standards for diagnosing septic arthritis. Hematologic abnormalities (increased leukocyte count and band count) are similar in both septic joint and transient synovitis. ESR and C-reactive protein (CRP) are more often elevated with septic arthritis but are nonspecific. Serum CRP rises more quickly than ESR in a patient with a septic joint, and it is the most useful test during the early stages. Radiographs may show effusion in either illness, and MRI is not indicated although ultrasonography may be helpful to detect an effusion.
7.
(B)
This is the classic presentation of SCFE (ie, a painful limp in an obese pubertal boy). The patient may complain of pain in the hip, thigh, or knee but on examination holds the leg in external rotation (see
Figure 55-2
).