Pediatric Examination and Board Review (203 page)
Read Pediatric Examination and Board Review Online
Authors: Robert Daum,Jason Canel

(C) polyhydramnios is a risk factor for poor lung development
(D) maternal use of angiotensin-converting enzyme (ACE) inhibitors may lead to polyhydramnios
(E) Potter syndrome is associated with polyhydramnios
3.
In the nursery, the neonate is fed a cow’s milk–based formula without any associated gagging or choking. At 15 hours of life, you are notified that this patient had one episode of bilious emesis. What is the next step in your evaluation?
(A) change to a soy-based formula
(B) continue feeds with close observation
(C) barium enema with anal manometry
(D) make the patient NPO
(E) abdominal and chest radiographs
4.
All the following are associated with polyhydramnios except
(A) prune belly syndrome
(B) fetal hydrops with anasarca
(C) esophageal atresia
(D) duodenal atresia
(E) multiple gestation
5.
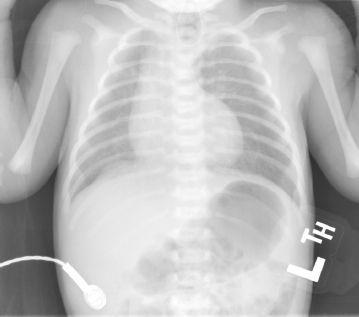
What is the radiographic finding on this x-ray (
Figure 113-1
)?
(A) double bubble
(B) multiple air fluid levels
(C) nonspecific bowel gas pattern
(D) thumbprinting
(E) all of the above
6.
What is your diagnosis based on the above radiographic finding?
(A) tracheal stenosis
(B) esophageal atresia without a distal fistula
(C) “H”-type tracheoesophageal fistula
(D) choanal atresia
(E) duodenal atresia
7.
What other organ systems or specific anomalies are associated with the above diagnosis?
(A) cardiac
(B) renal
(C) imperforate anus
(D) esophageal atresia
(E) all of the above
8.
What chromosomal anomaly or disease syndrome is most commonly associated with duodenal atresia?
(A) trisomy 13
(B) Turner syndrome
(C) trisomy 21
(D) trisomy 18
(E) Klinefelter syndrome
9.
Which statement is true of duodenal atresia?
(A) the pathophysiology is similar to that of other intestinal atresias
(B) abdominal distension is the most common presenting symptom
(C) duodenal atresia may present without bilious emesis
(D) duodenal atresia is not associated with an annular pancreas
(E) duodenal atresia is usually associated with oligohydramnios
10.
Which contrast study is indicated emergently in a baby with bilious vomiting?
(A) upper gastrointestinal (GI) series
(B) lower GI series
(C) head ultrasound
(D) ultrasound of the pylorus
(E) computed tomography of the abdomen
ANSWERS
1.
(A)
The normal amount of amniotic fluid at birth is 0.5-2 L. The volume is primarily determined by fetal urine output. Oligohydramnios is defined as an amniotic fluid volume less than 500 mL. Polyhydramnios is an amniotic fluid volume more than 2 L at birth. Oligo- and polyhydramnios are both associated with fetal anomalies and poor perinatal outcome. Assessment of amniotic fluid volume is done ultrasonographically by calculation of an amniotic fluid index (AFI), a summation of amniotic fluid volume in each of the four quadrants of the uterus. Oligohydramnios is defined as an AFI <5 cm, and polyhydramnios is defined as an AFI >24 cm.
2.
(A)
Amniotic fluid contains proteins, carbohydrates, lipids and phospholipids, urea and electrolytes, all of which aid in the growth of the fetus. In the late stages of gestation, amniotic fluid consists mostly of fetal urine. In utero, the fetus “inhales” amniotic fluid, allowing proper growth of lung tissue. Amniotic fluid also serves as a cushion to prevent trauma to the developing fetus and as a barrier to infection. Decreased fetal swallowing may lead to polyhydramnios. At term, the volume of amniotic fluid averages between 800 and 1000 mL. Maternal use of ACE inhibitors and Potter syndrome are associated with oligohydramnios.
3.
(D)
Bilious emesis in a newborn is a worrisome event and signals an obstruction distal to the ampulla of Vater. The first step in management of these patients is to make the patient NPO. The type of formula fed to the infant is not related to bilious emesis. If the neonate has not had a bowel movement after 48 hours, one would suspect Hirschsprung disease, and a barium enema with anal manometry would be part of the evaluation.
4.
(A)
Conditions associated with polyhydramnios:
• Idiopathic (2 of 3)
• GI anomalies → duodenal and esophageal atresia
• Central nervous system (CNS) anomalies → anencephaly, primary muscle disease
• Hydrops → immune and nonimmune
• Maternal diabetes
• Multiple gestation
• Other fetal anomalies
Conditions associated with oligohydramnios:
• Postterm gestation
• Chronic fetal hypoxia associated with severe preeclampsia
• Premature rupture of membranes
• Maternal dehydration
• Monochorionic twin gestation
• Potter syndrome
• Prune belly syndrome (Eagle-Barrett syndrome)
• Maternal use of ACE inhibitors
• Other fetal anomalies → renal-developmental or obstructive malformations
5.
(A)
The classic double-bubble sign represents air in the stomach (proximal to the atresia) and air in the first part of the duodenum (distal to the atresia) (
Figure 113-1
).
6.
(E)
Suspicion of duodenal atresia in the neonate would lead one to order an abdominal radiograph to look for the classic double-bubble sign, representing air in the stomach (proximal to the atresia) and air in the first part of the duodenum (distal to the atresia). If the chest radiograph showed the nasogastric tube coiled in a blind pouch in the neck, it would indicate a tracheal atresia. The nasogastric tube coiling in a blind pouch with air seen in the GI tract indicates a distal tracheoesophageal fistula (TEF). If there was no abdominal gas, it would indicate esophageal atresia without a distal TEF. TEF occurs in 1:3000-1:4500 live births. Polyhydramnios is present in about a third of cases with esophageal atresia. Babies with TEF present with excessive oral secretions shortly after birth that may lead to coughing, choking, and respiratory distress. Infants with an “H”-type TEF generally do not present in the newborn period.
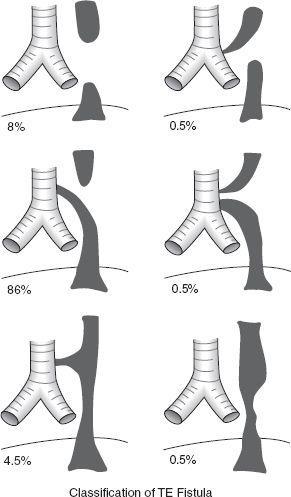
Figure 113-2
shows the various types of TEF. The most common is esophageal atresia with distal TEF.
7.
(E)
8.
(C)
Down syndrome (trisomy 21) is most commonly associated with duodenal atresia. Patau syndrome (trisomy 13) has the worst prognosis of all the trisomies. Holoprosencephaly, polydactyly, rockerbottom feet, neural tube defects, and heart defects are also frequent clinical features. Edwards syndrome is caused by trisomy 18. Multiple organ systems are involved in this syndrome, including GI anomalies, but duodenal atresia is not a classic feature.
9.
(C)
Whereas other atresias of the small and large bowel are isolated anomalies caused by mesenteric vascular accidents during later stages of development, duodenal atresia results from the failure of the epithelial solid cord to recanalize (failure of vacuolization). Bilious emesis is the most common presenting symptom of duodenal atresia. Rarely, the duodenal atresia may be proximal to the ampulla of Vater resulting in no bilious emesis. Annular pancreas is not an uncommon associated finding with duodenal atresia. Duodenal atresia is commonly associated with polyhydramnios.
10.
(A)
Bilious vomiting in an infant suggests a diagnosis requiring surgical therapy until proven otherwise. Immediate evaluation for malrotation should be done. The procedure of choice for diagnosis of malrotation is an upper GI series looking for the position of the duodenojejunal junction.
 S
S
UGGESTED
R
EADING