Anal Pleasure and Health: A Guide for Men, Women and Couples (19 page)
Read Anal Pleasure and Health: A Guide for Men, Women and Couples Online
Authors: Jack Morin Ph.d.

One manifestation of being overly serious about self-pleasuring is the feeling that masturbation must result in orgasm. Some people get so focused on coming that they hardly enjoy the journey. Masturbation doesn't have to lead anywhere; stop any time you want. And it's certainly better if you don't rush. Try taking breaks and maybe coming back to it later. This is a good way of becoming less goal-oriented and more pleasure-focused.
Erotic fantasies, typically a part of masturbation, can be a source of either joy or concern. This is especially true of fantasies involving anal intercourse. "Why is it," asks James, "that I like fantasizing about getting [anally] fucked, but I can't actually do it?" Ruth echoes the same concern: "When I think about it [anal intercourse], it's always a turn-on. I've even fantasized that Mel [her boyfriend] was really inside my anus during vaginal intercourse, especially when he enters from the rear; but every time we try anal sex it's no fun at all." One reason for James' and Ruth's apparent contradictions might be that they don't want to receive anal intercourse in actuality, even though they very much like it in fantasy. After all, there's no direct relationship between fantasy and behavior; people frequently fantasize things they would never want (or be able) to do. Another possibility is that James and Ruth would like to receive anal intercourse but are not yet comfortable with the reality. Either way, it's best if you can enjoy your fantasies just for themselves right now. Later, I'll suggest comfortable ways of discovering what-if anything-you'd like to try with a partner.
Other men and women discover that neither fantasy nor real-life anal stimulation is very erotic. Some even experience a decrease in excitement merely from thinking about it. If you're one of these people, as you become more familiar with anal fantasies and touch, you might become more interested. If you're genuinely willing, try deliberately introducing fantasies of anal stimulation at moments of high excitement. This approach may gradually help eroticize the anal area by replacing negative or neutral associations with positive ones.
Always remember the vast range of preferences expressed by humans in all spheres of life, certainly including sex. Nobody likes everything. Anal stimulation may simply not be erotic for you. If your partner wishes to play this way and you don't, the two of you will need to work out some sort of resolution (more on this in Chapter 11). As difficult as it can sometimes be, integrity requires that you speak your own truth.



The rectum is a tube-like structure made of loose folds of soft, smooth tissue. Its total length is about eight or nine inches. Normally the rectum is more open and spacious than the anus. But like the anus, it has a striking capacity to expand. The entire rectum is surrounded by muscles which, during a BM, contract and relax in wave-like motions-known as peristalsis-to move feces through the rectum and out the anal opening. The tension level of these muscles varies from person to person and reflects, among other things, individual emotional states and habitual muscular patterns. Chronic contractions of the rectal muscles contribute to constipation and other problems of the lower digestive tract. Rectal muscles are not nearly as powerful as the anal sphincters (except for one related muscle I'll discuss shortly). Nonetheless, if the rectal muscle are very tense, the insertion of an object or penis into it can easily become a pleasureless ordeal.
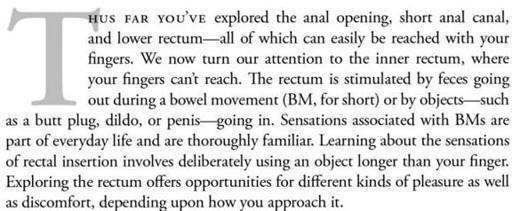
While the rectum is tube-like, it's not a straight tube. Instead it takes two curves along its length (see Figure 4). Knowledge of these curves is essential for the would-be rectal explorer. The lower rectum tilts forward toward the navel. After a few inches it curves in the opposite direction toward the backbone. This first curve is created by a strong, supportive muscle known as the pubo-rectal sling (shown in a detail of Figure 4). After another few inches the rectum curves slightly toward the front once again before joining the sigmoid (s-shaped) colon.
It's the first curve-and the underlying pubo-rectal sling muscle-that are most likely to make it difficult to receive an object or penis into the rectum. Figure 5 shows how an object entering the rectum at the wrong angle runs into the rectal wall at the first curve. If the object is inserted with force, it can cause pain. If a lot of force is used, a tear (fissure) in the rectal wall can result. Figure 5 also shows how a slight adjustment in the angle of entry easily prevents this. Difficulty in moving beyond the first curve can be exacerbated if the pubo-rectal sling muscle is constricted by tension, making the curve more pronounced and less flexible. The pubo-rectal sling, like all anal and rectal muscles, clamps down in response to fear, stress, chronic straining, pain, or improper diet.
The pubo-rectal sling is responsible for about 80% of continence, the ability to avoid the unwanted passage of feces or gas. Thus, even people with damaged anal sphincters can still retain a high degree of control. When a person feels the internal pressure associated with the need to defecate, the pubo-rectal sling contracts to hold back feces and gas until the first appropriate opportunity. Any pressure against the pubo-rectal sling-or at the upper end of the rectum where the colon starts-can trigger a similar holding-back response. Knowing this helps understand two phenomena commonly experienced when objects are inserted in the rectum: (1) the feeling of an imminent bowel movement even when this isn't going to happen, and (2) the tensing of the pubo-rectal sling, making insertion difficult and unpleasant. Clearly, these two experiences are related. Pressure from rectal insertion is perceived as an urge to defecate which, in turn, results in tensing of the pubo-rectal sling-a classic vicious cycle. Comfortable rectal insertion requires a reinterpretation of this response. This is relatively easy to do for most people because the sling can readily be brought under voluntary control, especially as you get more familiar with the other muscles of your pelvis. The key is to learn gradually, in a visceral way, that the urge to defecate isn't necessarily linked with the need for a BM. This awareness helps to relax the sling and gives your rectum maximum flexibility.
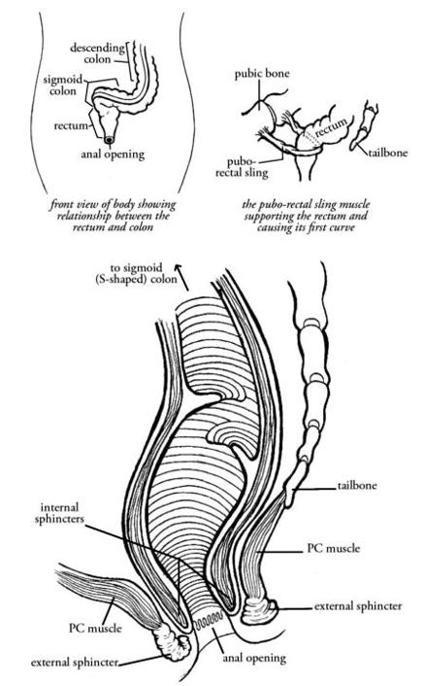
Figure 4. Anatomy of the Rectum
The second rectal curve is less pronounced and easily adaptable. Consequently, it's rarely a source of difficulty or discomfort during rectal insertion. When it does cause discomfort, slight adjustments in the angle of entry usually remedy the problem. It also helps to know that any position which places the legs at right angles to the upper body-such as sitting, squatting, lying on your back or side with knees pulled toward the chest, or on your knees in a "doggie" position-will straighten the rectum a bit. But no position completely eliminates the rectal curves.
Within this general description, rectal shape and size vary from person to person. Inserting objects into the rectum may be easier for one person in a particular position or at a certain angle of entry, while another position or angle is better for someone else. Differences are no doubt a combination of physiological variations and personal preference. Anyone who states that one position or angle is the best for rectal entry is over-generalizing from personal experience. There's no substitute for first-hand experimentation.
SOURCES OF PLEASURE DURING RECTAL STIMULATION. In comparison to the anus, the rectum contains relatively few nerve endings and is, therefore, less sensitive. The rectum has this in common with the vagina: the entryway is far more sensitive than the inner portion. Rectal nerves, like inner vaginal ones, primarily transmit sensations of pressure. Some people find these sensations immediately pleasurable, while others need to get used to them. More than a few men and women, however, report a remarkable sensitivity in their rectums. To some extent this sensitivity appears to be a learned capacity developed through paying attention. It certainly makes sense that the psychological enjoyment of rectal receptivity can greatly heighten the pleasure.
For men, stimulation of the prostate through the front of the rectal wall offers the potential of additional good sensations, as we saw in the last chapter. But there's more: Not too far in front of the anus is the interior "penile bulb," a highly sensitive area just below the surface of the perineum, the area between his scrotum and anus.
