Wallach's Interpretation of Diagnostic Tests: Pathways to Arriving at a Clinical Diagnosis (1124 page)
Authors: Mary A. Williamson Mt(ascp) Phd,L. Michael Snyder Md

BOOK: Wallach's Interpretation of Diagnostic Tests: Pathways to Arriving at a Clinical Diagnosis
10.33Mb size Format: txt, pdf, ePub
Renin-producing tumors of the kidney
TABLE 16–66. Differentiation of Primary and Secondary Aldosteronism Based on Blood Tests and Clinical Symptoms
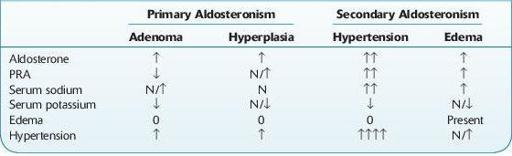
↑, increased; ↓, decreased; N, normal.
Decreased In
Other books
The Blood Pit by Kate Ellis
Bloodring by Faith Hunter
Sacrificed to the Dragon by Jessie Donovan
Carrier 02: Shadow of the Mark by Leigh Fallon
A Whole New Crowd by Tijan
Lion of Liberty by Harlow Giles Unger
Finding Her Fantasy by Trista Ann Michaels
Gilgamesh by Stephen Mitchell
Whistle by Jones, James