Wallach's Interpretation of Diagnostic Tests: Pathways to Arriving at a Clinical Diagnosis (560 page)
Authors: Mary A. Williamson Mt(ascp) Phd,L. Michael Snyder Md

BOOK: Wallach's Interpretation of Diagnostic Tests: Pathways to Arriving at a Clinical Diagnosis
9.28Mb size Format: txt, pdf, ePub
D, decreased; GFR, glomerular filtration rate; I, increased; N, normal; sl, slightly.
*when albuminuria is 0.075–0.1 g/d in IDDM, significant renal disease is present and albuminuria will progress to clinical nephropathy. GFR declines—10 mL/min/y after nephropathy is established.
Source: Selby JV, Fitz-Simmons SC, Newman M, et al. The natural history and epidemiology of diabetic nephropathy.
JAMA.
1990;263:1954–1960.
Who Should Be Suspected?
Diabetes and DN are more prevalent in blacks, Mexican Americans, Polynesians, and Maoris. Additional risk factors include poorly controlled diabetes, positive family history, and uncontrolled hypertension.
12-4
).
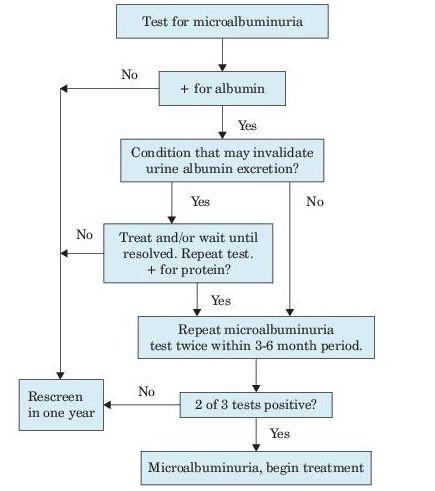
Figure 12–4
Screening for microalbuminuria.
Source: American Diabetes Association. Nephropathy in diabetes.
Diabetes Care
. 2004 Jan;27 Suppl 1:S79–83.
Suggested Readings
DOQI clinical practice guidelines and clinical practice recommendations for diabetes and chronic kidney disease.
Am J Kidney Dis.
2007;49(2 Suppl 2):S12–S154.
http://www.kidney.org/professionals/kdoqi/pdf/Diabetes_AJKD_FebSuppl_07.pdf
KDOQI clinical practice guideline for diabetes and CKD: 2012 update.
Am J Kidney Dis.
2012;60(5):850–886.
http://www.kidney.org/professionals/KDOQI/guidelines_diabetesUp/diabetes-ckd-update-2012.pdf
HENOCH-SCHÖNLEIN PURPURA NEPHRITIS
-
Schönlein purpura (HSP).
Other books
When I'm With You: The Complete Novel by Beth Kery
The Unlocked (Charlie Hartley Series Book 1) by Stonebridge, J.D.
Secrets Abound (Supernaturally Bound Book 1) by Erica Lee Cooke
Spin the Bottle by Rhian Cahill
Transcontinental by Brad Cook
Courting Lord Dorney by Sally James
Emma hearts LA by Keris Stainton
Taras Bulba and Other Tales by Vasilievich G Nikolai Vasilievich Gogol
The Sunset Warrior - 01 by Eric Van Lustbader
51 Shades of Maggie, Liverpool Style by Leesa Harker