Ross & Wilson Anatomy and Physiology in Health and Illness (49 page)
Read Ross & Wilson Anatomy and Physiology in Health and Illness Online
Authors: Anne Waugh,Allison Grant
Tags: #Medical, #Nursing, #General, #Anatomy

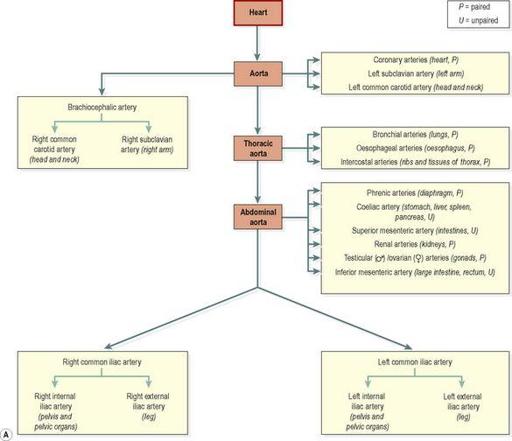
Figure 5.51
A.
The aorta and main arteries of the body.
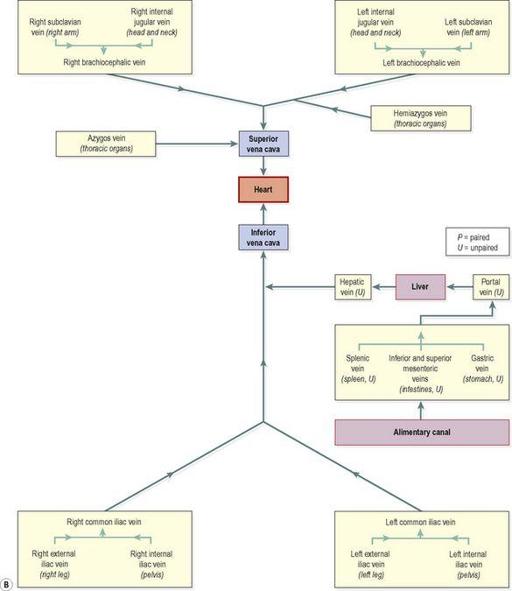
Figure 5.51
B.
The venae cavae and main veins of the body.
Fetal circulation

Learning outcomes
After studying this section, you should be able to:
outline the functions of the placenta
Features of the fetal circulation
The developing fetus obtains its oxygen and nutrients, and excretes its waste, via the mother’s circulation. To this end, both maternal and fetal circulations develop specific adaptations unique to pregnancy. Because the lungs, gastrointestinal system and kidneys do not begin to function till after birth, certain modifications in the fetal circulation divert blood flow to meet pre-natal requirements.
Placenta
This is a temporary structure that provides an interface between the mother and fetus, and allows exchange of substances between their circulatory systems. It develops from the surface of the fertilized ovum embedded into the maternal uterine endometrium (
Fig. 5.52
). It is expelled from the uterus during the final stage of labour soon after birth, when it is no longer needed.
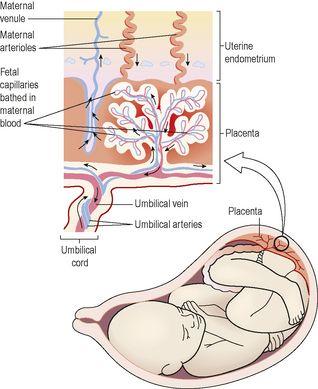
Figure 5.52
Structure of the placenta.
Structure
The mature placenta is pancake-shaped, weighs around 500 g, has a diameter of 20 cm and is about 2.5 cm thick, although wide individual variations occur. The placenta is firmly attached to the uterine wall and consists of an extensive network of fetal capillaries bathed in maternal blood. Whilst the fetal capillaries are in very close proximity to the maternal blood supply, the two circulations are completely separate. The placenta is attached to the fetus by a cord (the
umbilical cord
), which is usually about 50 cm long and contains two
umbilical arteries
and one
umbilical vein
wrapped in a soft connective tissue coat (
Fig. 5.52
). The cord enters the fetus at a spot on the abdomen called the
umbilicus
.
Functions
Placental functions include exchange of substances, protection of the fetus and maintenance of pregnancy.
Exchange of nutrients and wastes
Deoxygenated blood flows from the fetus into the placenta through the umbilical arteries, and travels through the network of fetal capillaries in the placenta. Because these capillaries are bathed in maternal blood, exchange of nutrients and gases takes place here and the blood that returns to the fetus in the umbilical vein has collected oxygen and nutrients and lost excess carbon dioxide and other wastes (
Fig. 5.52
).
Protection of the fetus
Temporary passive immunity (
p. 373
) lasting for a few months is provided by
maternal antibodies
that cross the placenta before birth.
Indirect exchange between the fetal and maternal circulations provides a ‘barrier’ to potentially harmful substances, including bacteria and drugs, although some may cross into the fetus, causing abnormal development. They include:
•
alcohol
•
some infective agents, e.g. the virus that causes German measles (rubella)
•
other substances and some drugs, which are then known as
teratogens
.
Maintenance of pregnancy
The placenta has an essential endocrine function because it secretes the hormones that maintain pregnancy.
Human chorionic gonadotrophin (hCG)
This hormone is secreted in early pregnancy, peaking at around 8 or 9 weeks and thereafter in smaller amounts. hCG stimulates the
corpus luteum
(
Ch. 18
) to continue secreting progesterone and oestrogen which prevent menstruation and maintain the uterine endometrium, sustaining pregnancy in the early weeks (see
Fig. 18.10, p. 444
).
Progesterone and oestrogen
As pregnancy progresses, the placenta takes over secretion of these hormones from the corpus luteum, which degenerates after about 12 weeks. From 12 weeks until delivery, the placenta secretes increasing levels of oestrogen and progesterone. These hormones are essential for maintenance of pregnancy.
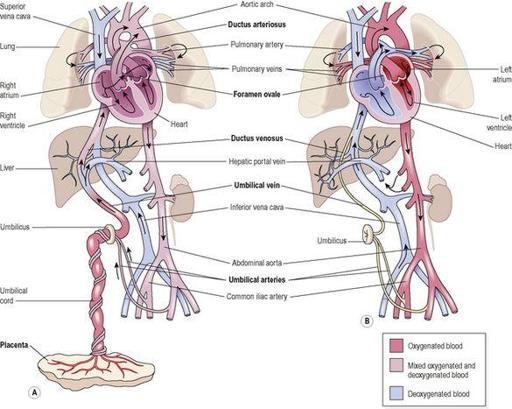
Fetal adaptations (
Fig. 5.53A
)
Ductus venosus
This is a continuation of the umbilical vein that returns blood directly into the fetal inferior vena cava, and most blood, therefore, bypasses the non-functional fetal liver.