Ross & Wilson Anatomy and Physiology in Health and Illness (53 page)
Read Ross & Wilson Anatomy and Physiology in Health and Illness Online
Authors: Anne Waugh,Allison Grant
Tags: #Medical, #Nursing, #General, #Anatomy

Figure 5.58
Arteriosclerotic arteries.
When small arteries (arterioles) are involved, their lumen is reduced because of a deposition of a substance called
hyaline material
, which also reduces the elasticity of the vessel wall. Because these arteries are the main determinants of peripheral resistance (
p. 76
), this narrowing increases peripheral resistance and blood pressure. Damage to small vessels has a disproportionate effect on blood flow, leading to ischaemia of tissues supplied by affected arteries. In the limbs, the resultant ischaemia predisposes to gangrene, which is particularly serious in people with diabetes mellitus.
Senile arteriosclerosis
This is a condition affecting elderly people. Progressive loss of elasticity and reduced arterial lumen lead to cerebral ischaemia and loss of mental function. There may or may not be evidence of hypertension.
Aneurysms
Aneurysms are abnormal local dilations of arteries, which vary considerably in size (
Fig. 5.59
). Predisposing factors include atheroma, hypertension and defective formation of collagen in the arterial wall.
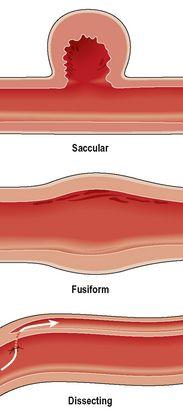
Figure 5.59
Types of aneurysm.
Complications of aneurysm
If an aneurysm ruptures, haemorrhage follows, the consequences of which depend on the site and extent of the bleed. Rupture of the aorta is likely to be fatal, while bleeding into the subarachnoid space can also cause death, or permanent disability. Aneurysm damages the blood vessel endothelium, making it rougher than usual, which increases the risk of clot formation. Clots may block circulation locally, or elsewhere if they travel in the bloodstream as emboli. In addition, the swelling associated with the distended artery can cause pressure on local structures such as other blood vessels, nerves or organs.
Types of aneurysm
Fusiform
or spindle-shaped distensions occur mainly in the abdominal aorta and less commonly in the iliac arteries. They are usually associated with atheromatous changes.
Saccular
aneurysms bulge out on one side of the artery. When they occur in the relatively thin-walled arteries of the circulus arteriosus (circle of Willis,
p. 96
) in the brain they are sometimes called ‘berry’ aneurysms. They may be congenital, or be associated with defective collagen production or with atheromatous changes.
Dissecting
aneurysms occur mainly in the arch of the aorta, caused by infiltration of blood between the endothelium and tunica media, beginning at a site of endothelial damage.
Microaneurysms
are fusiform or saccular aneurysms, occurring in small arteries and arterioles in the brain. They are associated with hypertension. Recurring small strokes (
transient ischaemic attacks
) are commonly due to thrombosis in the aneurysm or to haemorrhage when an aneurysm ruptures.
Venous thrombosis
The risk factors predisposing to a clot developing within a vein are discussed on
page 113
.
Venous thrombosis may be
superficial thrombophlebitis
, which usually resolves spontaneously, or
deep vein thrombosis
.
Superficial thrombophlebitis
In this acute inflammatory condition a thrombus forms in a superficial vein and the tissue around the affected vein becomes red and painful. The most common causes are:
•
intravenous infusion
•
varicosities in the saphenous vein.
Deep vein thrombosis (DVT)
A thrombus forms in a deep vein commonly in the lower limb, pelvic or iliac veins, but occasionally in an upper limb. The thrombus may affect a long section of the vein and, after some days, fibrinolysis (
p. 64
) may enable recanalisation through the blockage. Deep vein thrombosis may be accompanied by pain and swelling, but is often asymptomatic.
The commonest complication of DVT is pulmonary embolism (
p. 112
), which is often fatal.
Varicose veins
A varicosed vein is one that is so dilated that the valves do not close to prevent backward flow of blood. Such veins lose their elasticity, become elongated and tortuous, and fibrous tissue replaces the tunica media.
Predisposing factors
•
Heredity – there appears to be a familial tendency.
•
Gender – females are affected more than males.
•
Pregnancy.
•
Age – the progressive loss of elasticity in vein walls that accompanies increasing age leads to less efficient elastic recoil.
•
Reduced efficiency of the skeletal muscle pump (
p. 86
), as in prolonged standing/sitting, or obesity, where excess adipose tissue around veins does not give adequate support.
•
Pressure – because of their thin walls, veins are easily compressed by surrounding structures, leading to increased venous pressure distal to the site of compression.
Sites and effects of varicose veins
Varicose veins of the legs
When valves in anastomosing veins between deep and superficial leg veins become incompetent, the venous pressure in the superficial veins rises. In the long term they stretch and become chronically dilated because the superficial veins are less well supported by surrounding tissues than deeper ones. Such areas show through the skin as
varicose veins
(
Fig. 5.60
). The great and small saphenous veins and the anterior tibial veins are most commonly affected, causing aching and fatigue of the legs, especially during long periods of standing. These dilated, inelastic veins rupture easily if injured, and haemorrhage occurs.
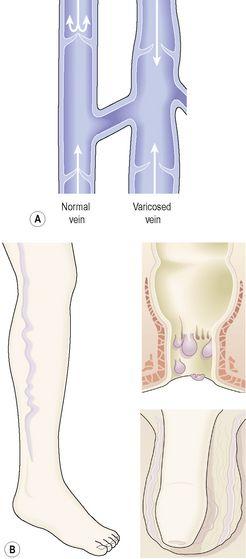
Figure 5.60
A.
Normal and varicosed veins.
B.
Common sites for varicosities – the leg, scrotum (varicocele) and anus (haemorrhoids).
The skin over a varicose vein may become poorly nourished due to stasis of blood, leading to the formation of
varicose ulcers
, usually on the medial aspects of the leg just above the ankle.
Haemorrhoids
Sustained pressure on the veins at the junction of the rectum and anus leads to increased venous pressure, valvular incompetence and the development of haemorrhoids (piles,
Fig. 5.60
). The most common causes are chronic constipation, and the increased pressure in the pelvis towards the end of pregnancy. Slight bleeding may occur each time stools are passed and, in time, may cause anaemia. Severe haemorrhage is rare.
Scrotal varicocele
Each spermatic cord is surrounded by a plexus of veins that may become varicosed (
Fig. 5.60
), especially in men whose work involves standing for long periods. If the varicocele is bilateral, the increased temperature due to venous congestion may depress spermatogenesis and cause infertility.
Oesophageal varices
Raised pressure in the lower oesophageal veins can rupture them, leading to a potentially fatal hamorrhage (
p. 313
).
Tumours of blood and lymph vessels
Angiomas
Angiomas are benign tumours of either blood vessels (haemangiomas) or lymph vessels (lymphangiomas). The latter rarely occur, so angioma is usually taken to mean haemangioma.
Haemangiomas
These are not true tumours, but are sufficiently similar to be classified as such. They consist of an excessive growth of blood vessels arranged in an uncharacteristic manner and interspersed with collagen fibres.
Capillary haemangiomas
Excess capillary growth interspersed with collagen in a localised area makes a dense, plexus-like network of tissue. Each haemangioma is supplied by only one blood vessel and if it thromboses, the haemangioma atrophies and disappears.
Capillary haemangiomas are usually present at birth and are seen as a purple or red mole or birthmark. They may be quite small at birth but grow at an alarming rate in the first few months, keeping pace with the growth of the child. After 1 to 3 years, atrophy may begin, and after 5 years about 80% of tumours have disappeared.
Cavernous haemangiomas
Blood vessels larger than capillaries grow in excess of normal needs in a localised area and are interspersed with collagen fibres. They are dark red in colour and may be present in the skin, though more commonly in the liver. They grow slowly, do not regress and may become large and unsightly.
Oedema

Learning outcomes
After studying this section, you should be able to:
define the term oedema