Resurrecting Pompeii (33 page)
Read Resurrecting Pompeii Online
Authors: Estelle Lazer

Healed depressed fracture of a skull (TdS 199), displaying involvement of both the inner and outer tables. View of the outer table
 Figure 8.7
Figure 8.7Inner table of a skull (TdS 199) with a healed depressed fracture
A healed injury was also observed on the right parietal bone of a skull stored in the Forum Baths.
73
It is approximately oval in shape and covers an area of 30 x 10 mm. The affected area presents as an oval region of granulated healing bone, which is ringed by a scar-like bony ridge. It is about 50 mm to the right of the sagittal suture. The outer table and inner tables are both involved though it is only just visible on the inner table. The injury has healed completely with no sign of secondary infection. It has been interpreted as being consistent with a wound resulting from a blow to the head.
74
Apart from these cases there were two left femora that displayed pathological changes that were consistent with trauma, but interpretation required confirmation from histological and/or x-ray analysis. Two
75
appeared to exhibit healed fractures, one
76
of which was consistent with a bending fracture on the proximal third of the shaft.
77
Another left femur
78
exhibited major changes to the femoral head and a shortening of the neck, which could variously be interpreted as a slipped femoral capital epiphysis as a result of a stress fracture, though the most likely interpretation is hip displacement, Perthes’ disease or osteoarthritis to the head with extensive remodelling and shortening of the neck. Osteoarthritic changes could have been the result of displacement or dislocation as the articular cartilage would have been compromised and would not have been nourished by the synovial fluid, which in turn would have caused the cartilage to break down and the commencement of osteophytic change to the bone.
79
A number of bones show evidence of osteophytic change (see below). Interpretation of such changes usually requires an examination of the entire skeleton to establish whether they were the result of arthropathy or trauma. It is possible that some of the osteophytic change, such as the presence of lipping and eburnation on the distal condyles of 11 of the sample of about 320 left and right femora in the Forum Bath collection, may reflect trauma. This interpretation may be supported by the fact that most of these cases display no signs of osteophytic change at the femoral head. It is possible that the local roads, with their deep gutters and unevenly worn stone blocks, ridged with ruts from carriage wheels, could have contributed to such injuries.
The perimortem skull fracture
80
is likely to have been the cause of death of this individual. The radius, ulna and tibia that had healed without displacement
81
would probably not have had an appreciable effect on the individuals associated with them and certainly would not have prevented their departure from Pompeii. While having a shorter leg would not have been an asset, it would probably not have impeded the escape of these individuals associated with the healed compound leg fractures
82
in the considerable period of time
83
associated with the first phase of the eruption.
The impact of the depressed fracture
84
requires further consideration. A fracture of this magnitude, with its involvement of both the tables, is likely to have resulted in some damage to the brain. The area involved corresponds with Broca’s area of the brain, which is concerned with the production of speech. It is notable that for most humans the location of the main language centre is in the left hemisphere of the brain. This is almost independent of handedness, which means that language was probably the function that was affected in this individual regardless of which hand they favoured. The person who sustained these injuries would have had a problem with syntax, especially in relation to the generation of sentences. It is possible that another portion of the brain may have taken over this function over time. It is unlikely that this injury would have hampered the escape of an individual from the erupting volcano.
85
Only one unequivocal case of surgical intervention was observed in the sample. This took the form of a trephination on a skull,
86
which from the degree of healing, had been performed a considerable time prior to death (Figure 8.8). The perforation associated with the surgery is surrounded by an almost circular region of granulated healing bone which, in turn, is ringed by a scar-like bony ridge. Both tables are involved, though the surface of the inner table is not raised. This suggests that the injury is not a depressed
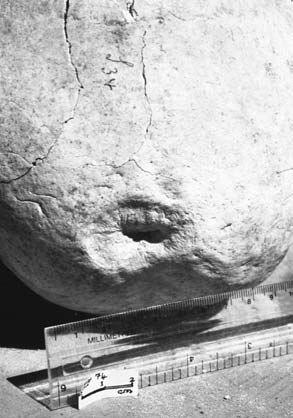 Figure 8.8
Figure 8.8Healing trauma, interpreted as a trephination on the skull of individual (TF 74) with hyperostosis frontalis interna
fracture. The bone defect is about 4 x 1 mm. It is in the middle of a depression about 2.5 mm below the normal surface of the surrounding parietal bone. This depression is two stepped and oval in shape. The outer ring measures about 35 x 25 mm. The inner ring is more circular in shape and covers an area of 20 x 20 mm. Elongated growths of healing bone do not quite bridge the defect. There is no sign of secondary infection. The changes observed on this bone are all consistent with a healing trephination.
Trephination, or trepanation, is a surgical procedure that involves incision of the scalp, followed by cutting the skull, often into a circular shape to make a hole and the excision of bone. While most scholars use the terms interchangeably, the distinction between trepanation and trephination is that the former is more general and refers to an opening of the cranium made by any instrument or procedure, whilst the latter specifically relates to the surgical removal of a disk of bone. There is evidence in the skeletal record that this operation has been performed, often successfully, over a wide geographical area for many millennia. It is a very dangerous procedure as it ultimately involves exposure of the cranial cavity to the external environment, though before the problem of potential infection is faced, the surgeon has to avoid damage to the dura mater, which, if perforated, would result in fatal leakage of the cerebrospinal fluid in which the brain floats. The meninges, brain and blood vessels also have to be avoided for the patient to survive the operation.
From the degree of healing, it can be established that the trephination was performed a considerable time before death. The long-term survival of this individual with no sign of osteomyelitis is not uncommon for archaeological cases of trephination. It has been suggested that one of the reasons for the high success rate was the high vascularity of the soft tissue that overlies the cranial vault, which would have decreased the likelihood of secondary infection. The lack of observed infection also indicates the use of clean instruments for this procedure. It is notable that the operation was performed on the left parietal bone. No satisfactory explanation has been established for the observation that most archaeological cases of trephination involve the left frontal or parietal bones.
87
While there is minimal evidence of surgical intervention in the Pompeian skeletal sample, discoveries of other classes of archaeological material, like medical implements, indicate that it was practised more widely in the Campanian settlements. In Pompeii alone, medical instruments have been identified with certainty at 21 sites and equivocal examples at a further 6. In addition, finds of small collections of about ten tools have been interpreted as home medical kits used for the treatment of minor injuries and ailments.
The range of instruments discovered is impressive and includes scalpels, specula, catheters, tweezers, probes and implements for cauterizing. Identifi- cation of these instruments has largely been based on the considerable documentary evidence for the use of surgical procedures in the Roman Empire in the form of medical texts. The most useful for the Pompeian material is the
De Medicina
of Celsus, which was written in Italy during the reign of Tiberius. In addition, much medical equipment remained virtually unchanged in form until the first part of the twentieth century and function was easily established by medical practitioners in the late nineteenth and early twentieth centuries.
88
Some of the instruments that have been found in excavations of the Vesuvian sites would have specifically been used to treat bones. For example, two bone elevators were identified in the collection that is now housed in the Naples museum, and records suggest that another one or two were discovered in Pompeii prior to 1826 but have subsequently been lost. Like most of the medical implements found in Pompeii, these were made of copper alloy and had a handle with an arched rectangular plate at each end. The plates were smooth on the outside and serrated on the inner surface to assist with grip. A bone elevator, or
vectis
, was used to lever fractured bones into position so that they could heal without distortion. Bone elevators could also be used to raise depressed bone and it has been suggested that they may have been used to facilitate tooth extraction. As there is no clear evidence that bone files have been discovered at the site, it has been argued that the serrated edges of the bone levers could also have been used for this function.
89
About ten implements found in the Campanian excavations have been interpreted as chisels. The exact provenance is not known for a number of these pieces and interpretation is hampered by the fact that they tend to be represented by the bronze handles, rather than the blades, which would have been made of iron or steel, and have not survived. The function of the bone chisel or
scalper
is largely known through ancient medical writers, like Celsus,
90
who describes their use for the removal of diseased or fractured bones, especially from the cranium. He also mentions their application for smoothing out projecting bone from compound fractures after it was filed or cut.
91
Apparently, this tool was also employed for the removal of additional digits. It is notable that the bone chisel was generally smaller than those used for carpentry but it was possible that carpenter’s chisels could also be employed for surgical use.
92
According to Bliquez,
93
the discovery of such tools suggests that surgeons in the Campanian region were equipped to treat severe fractures. In view of this, it is interesting to note that a number of instruments that might have been expected as part of the bone surgeon’s tool kit, such as gouges, bone files, drills and saws, have, so far, not been discovered at Pompeii. It is possible that these tools did not survive as they were made of materials that were not durable in an archaeological context, such as steel, though Bliquez is doubtful that this provides a sufficient explanation. It is possible that the full repertoire of tools has just not yet been excavated.
94
Though drills, trephines and saws have not been discovered in Pompeii, Roman methods of trephination deserve a brief consideration in relation to the interpretation of the healing surgical procedure on the skull described above.
95
Bow-drills were often used for treatment of diseases or injuries to the skull. They were made of a straight steel or bronze rod with a rotating handle at the upper end and a steel augur or circular saw at the lower end. A piece of cord was attached and passed tightly around the drill. The augur or saw was placed against the bone and was rapidly rotated by the movement of the bow drill, which enabled rapid perforation of the bone. For the removal of small circular pieces of bone, the augur was replaced by a crown trephine or
modiolus
, which was a short steel tube with teeth at the lower end. After a disc of bone was excised, the edges of the hole were cut back with the chisel until healthy bone was revealed. Celsus
96
writes about the use of an instrument to protect the membrane that surrounds the brain during this type of surgery. It is possible that this was a version of a double blunt hook. The instrument was pushed under the bone that was to be removed as a guard to prevent the chisel penetrating the membrane.
97
In view of the documentary and archaeological evidence for medical knowledge and practice in the Roman era, it perhaps seems remarkable that there was no apparent attempt to set the compound fractures of the femur and tibia and fibula.
98
There are a number of possible explanations for this. One is that these injuries might have been sustained in a geographical region where medical attention was not available. Another is that these individuals may not have had access to medical practitioners for financial or social reasons.
The frequency of trauma in the entire bone sample that could be identi fied from gross inspection was about 0.6 per cent. If the 11 cases of osteophytic change to the distal articular surface of the femur could be demonstrated to have resulted from trauma, the percentage would rise to 1.2 per cent. The rate of observed trauma in the radius and ulna was 0.5 per cent. For the tibia and fibula it was also 0.5 per cent and 0.8 per cent for the femur. If the additional eleven equivocal cases were added the frequency for trauma to the femur would rise to 3 per cent.
Bisel documented the cases of trauma that she observed in the Herculaneum sample that was available to her, though she did not distinguish between fractures, dislocations and inflammatory responses. This makes it difficult to compare her results with the Pompeian data. She reported that 32 per cent of the male sample and 11.4 per cent of the female sample displayed evidence of trauma, with a population average of 22.7 per cent. She did not consider that these figures indicated bias towards injury in the Herculaneum sample.
99
Capasso recorded cases of fractures separately from evidence of other types of trauma. He reported 31 fractures in 17, or about 10.5 per cent, of the 162 individuals that he studied. Like Bisel, he found the majority of cases involved males, with a ratio of 4.7: 1. He attributed the higher incidence of fractures in males to gender-related division of labour. Four of the fractures involved the frontal bone of the skull, one the temporal bone, one the nasal region and one mandible. There were three fractures of the radius, four of the ulna, one of the humerus and one of the femur. It is notable that Capasso had access to x-ray technology for his study.
100
It could be misleading to compare the Pompeian figures for the frequency of fractures with those obtained from other archaeological sites and modern populations as many of these studies would have utilized x-ray technology, and in the case of modern living populations, there is the advantage that all the skeleton is available for investigation. Bearing this in mind, it is instructive to make a brief survey of fracture rates in archaeological samples for comparison with the Pompeian results as they seem rather low compared to those from Herculaneum.
A fracture rate of between 1.0 and 3.6 per cent was reported for Greek and Turkish skeletal samples, dating from the seventh millennium to the second century
AD
. A 1.8 per cent rate of bone fracture was observed for a prehistoric central Californian population, the skeletons from the Libben site in Ohio had a 3 per cent fracture frequency and skeletal samples from various medieval British sites showed a range of between 0.3 to 6 per cent. Similarly, a visual survey of 6000 Egyptian skeletons revealed that about 3 per cent of the sample had sustained fractures. The bones most commonly affected are those of the arm, especially the forearm. Fractures to the femur tend to be fairly uncommon in most archaeological skeletal samples, as are fractures to the tibia and fibula.
101
The Pompeian figures are a little lower than most of the above-mentioned populations, but still within the range that has been observed for numerous archaeological sites, whilst the figures from Herculaneum are somewhat higher. It is possible that the survival of complete skeletons and the use of radiography has contributed more to the disparity in observed frequency than possible skewing towards disability. Fifteen of the fractures observed in the Herculaneum sample involve ribs, carpals, metacarpals, tarsals and metatarsals, bones which generally did not survive in the disarticulated Pompeian sample. The possibility of sample bias must also be considered. Ciprotti, for example, mentions the removal to the museum in Naples in the nineteenth century of a femur that demonstrated pathological changes and while it is likely that there were other cases, this activity probably would not have had a significant effect on the post-cranial sample.
102
Attention was usually focused on crania in the nineteenth century and they were more likely to be collected. The use of femora for hinge manufacture (see Chapter 5) is unlikely to have contributed to the loss of bones affected by trauma as pathological cases would not have been selected for this purpose since the hinges needed to be as close to perfect cylinders as possible.
Even though the available Pompeian sample does not re flect the entire corpus of excavated human skeletal material, it appears that it is random, with the exception of femora. Though some bones with pathology may have been selectively removed in the nineteenth century, there is no evidence for the removal of specific bones in the major part of the twentieth century. The frequency of observed trauma in the Pompeian skeletal collection is low, which indicates that the sample was not biased towards the infirm. There was no sign of any infirmity in the sample that would have absolutely prevented an unaided escape from the eruption. In fact, it appears unlikely that most of the cases of healed trauma would have had a significant impact on the survival prospects of these people. It is possible, however, that the decision of a few individuals to either flee or remain in Pompeii may have been influenced by the effects of pathology that had resulted in impaired mobility, as in the case of the individual with the malaligned healed compound fractures of the tibia and fibula.
103
The cases of healed trauma in the Pompeian sample are testimony to the robust immune systems of these individuals.