Read Pediatric Primary Care Case Studies Online
Authors: Catherine E. Burns,Beth Richardson,Cpnp Rn Dns Beth Richardson,Margaret Brady
Tags: #Medical, #Health Care Delivery, #Nursing, #Pediatric & Neonatal, #Pediatrics
Pediatric Primary Care Case Studies (62 page)

A discussion with the family about the evaluation for causes and the symptomatic treatment of the IM is important. Points that are raised in the discussion include:
Explanation of the diagnosis, the variability of the course of IM, and the lack of specific treatment for IM.
The family wants to know the exact cause of Maya’s illness because there are four other children in the household and more than 20 cousins whom the family sees on a regular basis. After discussion of the treatment plan, Maya’s mother is instructed to get the lab work done in 2 days to increase the specificity of the testing. The results from day 8 of the illness show a negative Monospot test with a CBC with 78% lymphocytes and 18 atypical lymphocytes. The child returns on day 10 of illness with a predominance of fatigue and fever. The child still complains of a sore throat and painful lymph nodes. The physical examination is unchanged and no hepatosplenomegaly is found. You decide to do additional laboratory testing. Liver function tests and EBV-specific antibodies are ordered to confirm the suspected diagnosis of EBV mononucleosis.
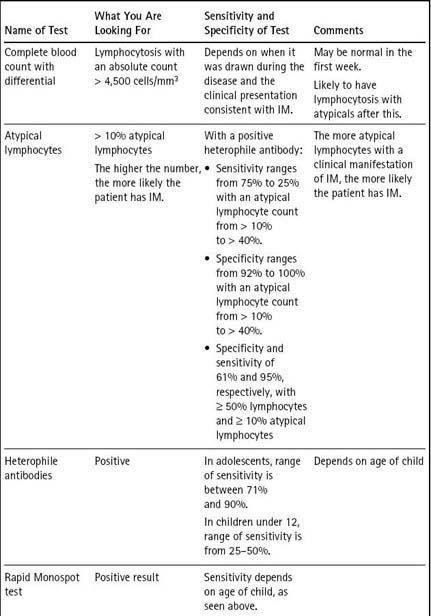
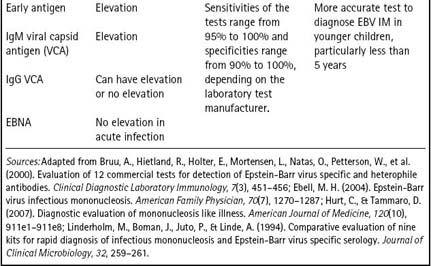
EBV-specific antibodies include IgM and IgG against the viral capsid antigen (VCA), Early antigen (EA) diffuse staining, and EBV nuclear antigen (EBNA). The two tests that are most helpful in diagnosing active and recent infections are the IgM anti-VCA and the EA. IgM levels go up in acute infection and decrease over 3 months. Early antigens are present at the onset of clinical illness and decrease as the infection resolves, usually over 6 weeks. Early antigens are not present once the symptomatic period is ended. Another antibody that can be assayed is IgG antibodies to viral capsid antigen, which will rise 6 to 12 weeks following the EBV infection and remain elevated for life (Ebell, 2004). EBNA are long-term antibodies that do not rise until several weeks to months after the onset of infection. These are not found in acute infection and are a marker of EBV infection in the past (Pickering et al., 2006).
CMV can also cause elevation of the IgM antibodies to VCA. The sensitivities of the tests range from 95% to 100% and the specificities of the test range from 90% to 100%, depending on the laboratory test manufacturer (Bruu et al., 2000).
The results of laboratory testing done on day 10 of Maya’s illness are back. The child’s tests for IgM VCA, EA, IgG VCA, and EBNA are all negative. The aminotransferases (AST and ALT) are both elevated five times above normal, reflecting a mild hepatitis. The bilirubin and alkaline phosphatase levels are within normal limits, indicating no biliary obstruction. The family is called with the results of the serology and is asked to return in 2 days for reevaluation. At this time, the fever is starting to come down but the fatigue persists. The diagnosis of EBV-negative mononucleosis is considered, and given the attendance at a daycare center after-school program and the predominance of fatigue and fever in the presentation, CMV serology for anti-CMV IgM and IgG is ordered (see
Table 16-3
). The family persists in wanting to know the exact cause of the illness and wants the additional serology tests done. The plan is to continue to symptomatically treat the child’s fever with Advil, allow for rest, provide fluids and foods the child can tolerate, keep the child home from school, limit rough play, and maintain infection control measures to prevent household spread.
Table 16–3 Laboratory Testing in Infectious Mononucleosis (IM)