Pediatric Examination and Board Review (69 page)
Read Pediatric Examination and Board Review Online
Authors: Robert Daum,Jason Canel

(C) androgen receptor
(D) 21-hydroxylase
(E) all of the above
12.
What structures do the Müllerian ducts form?
(A) fallopian tubes, uterus, and upper vagina
(B) ovaries, fallopian tubes, and uterus
(C) fallopian tubes, uterus, and upper and lower vagina
(D) ovaries, uterus, and upper vagina
(E) ovaries, uterus, and cervix
13.
What structures do the Wolffian ducts form?
(A) epididymis, vas deferens, penile urethra
(B) testes, epididymis, vas deferens
(C) testes, epididymis, seminal vesicles
(D) epididymis, seminal vesicles, penile urethra
(E) epididymis, vas deferens, seminal vesicles
14.
What is the role of Leydig cells in sexual differentiation?
(A) cause testicular enlargement
(B) produce testosterone, which stabilizes the Wolffian ducts
(C) enhance Sertoli cell formation
(D) cause regression of the Müllerian ducts
(E) spermatogenesis
15.
Growth and differentiation of the external genitalia in males depends most on which of the following?
(A) testosterone
(B) Müllerian-inhibiting hormone
(C) LH and follicle-stimulating hormone (FSH)
(D) SRY
(E) dihydrotestosterone
16.
Infants born with 5-alpha-reductase deficiency have which of the following features?
(A) 46,XX, male internal genitalia, female external genitalia
(B) 46,XY, male internal genitalia, female external genitalia
(C) 46,XX, female internal genitalia, male external genitalia
(D) 46,XY, female internal genitalia, male external genitalia
(E) 46,XY, female internal genitalia, female external genitalia
17.
At what age do females need to be exposed to excess androgens to cause labial fusion and development of a urogenital sinus (
Figure 43-2
)?
(A) before 4 weeks’ gestation
(B) between 4 and 12 weeks’ gestation
(C) between 12 and 16 weeks’ gestation
(D) between 16 and 24 weeks’ gestation
(E) after 24 weeks’ gestation
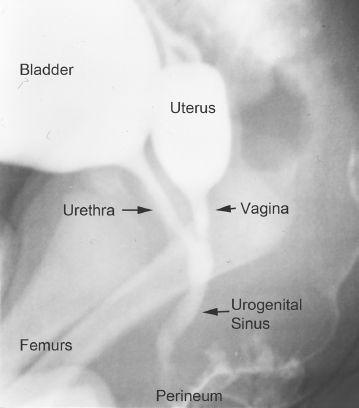
FIGURE 43-2.
Retrograde urethrogram of the internal genitalia of a virilized female infant with congenital adrenal hyperplasia as a result of 21-hydroxylase deficiency. With early exposure to androgens, the urethra and vagina do not extend to the perineum to form separate openings. An internal connection between the urethra and vagina forms a urogenital sinus, which results in only a single opening on the perineum.
18.
What is the lower limit of normal penile length in a male term newborn?
(A) 1.5 cm
(B) 2.0 cm
(C) 2.5 cm
(D) 3.0 cm
(E) 3.5 cm
19.
In females, the genital tubercle becomes which of the following?
(A) clitoris
(B) labia minora
(C) labia majora
(D) vaginal opening
(E) vagina
ANSWERS
1.
(C)
CAH, which is the most common diagnosis in virilized 46,XX infants. The ambiguous genitalia in female infants is caused by excess androgen exposure in utero and can range from mild virilization with posterior fusion to complete virilization. Maternal androgen exposure and ovotesticular DSD can both cause excess virilization in girls, but they are not as common as CAH. 5-alpha-reductase deficiency and gonadal dysgenesis cause genital ambiguity in males.
2.
(C)
21-Hydroxylase deficiency. 21-Hydroxylase deficiency caused by mutations in the 21-hydroxylase gene accounts for most of CAH. A deficiency of 21-hydroxylase impairs the conversion of 17-hydroxyprogesterone to 11-deoxycortisol, resulting in decreased cortisol production, and impairs the conversion of progesterone to deoxycorticosterone, resulting in defects in aldosterone production. Males with 21-hydroxylase deficiency do not present with genital ambiguity. However, males with 3-beta-hydroxysteroid dehydrogenase deficiency, 17-alpha-hydroxylase deficiency, and StAR deficiency are undervirilized.
3.
(E)
Possibility of a salt-wasting crisis. Children with CAH as a result of 21-hydroxylase deficiency can produce inadequate aldosterone leading to a salt-wasting crisis. Infants with a salt-wasting crisis present with failure to thrive, lethargy, vomiting, hypotension, hypovolemia, hyponatremia, and hyperkalemia. If CAH is not diagnosed and treated promptly, it can be fatal. Newborn screening programs have allowed the early detection of CAH as a result of 21-hydroxylase deficiency, especially in boys who do not present with ambiguous genitalia, and mildly virilized girls. Stress doses of hydrocortisone should be given to all infants in whom a diagnosis of CAH is considered. This will provide both glucocorticoid and mineralocorticoid coverage. Once infants with salt-wasting CAH are put on maintenance hydrocortisone, a mineralocorticoid must be added. Approximately two-thirds of infants with CAH are salt wasters.
4.
(B)
25%. Congenital adrenal hyperplasia as a result of 21-hydroxylase deficiency is transmitted as an autosomal recessive trait. Thus, assuming she has more children with the same father, there is a 25% chance that they will inherit both mutant alleles and be affected with CAH. It is possible to diagnose children prenatally. In subsequent pregnancies, this mother can be started on dexamethasone early in the pregnancy (by 5-6 weeks) to attempt to lessen the degree of genital ambiguity in affected female offspring by lowering the excess androgen production. Screening for CAH is done either by chorionic villus sampling or amniocentesis. Dexamethasone is only continued in women carrying affected female fetuses. The excess androgen production in affected males in utero currently has no known detrimental effect.
5.
(A)
17-Hydroxyprogesterone. The most common enzyme deficiency causing CAH is deficiency of 21-hydroxylase, which converts 17-hydroxyprogesterone to 11-deoxycortisol. Thus a deficiency of 21-hydroxylase will lead to a buildup of the precursor, 17-hydroxyprogesterone.
6.
(B)
Panhypopituitarism. This describes a baby with micropenis. The presence of other midline defects suggests panhypopituitarism. Pituitary gonadotropins are necessary for phallic enlargement after the external genitalia are formed. This baby must be screened for other pituitary hormone deficiencies. CAH is a less likely cause of genital ambiguity when other nongenital anomalies are present. Patients with ovotesticular DSD have the presence of both female and male internal genitalia with dysgenetic or mixed gonads.
7.
(E)
Karyotype, pelvic ultrasound, measurement of adrenal steroids. Determination of the karyotype can help classify the infant as an undervirilized male, a virilized female, or a mixed sex chromosome pattern. Ultrasound of the pelvis can help determine the presence of the gonads, uterus, and vagina. Measurement of adrenal steroids is necessary because CAH is a common cause of ambiguous genitalia, and patients can have life-threatening adrenal insufficiency if not diagnosed and treated. Biopsy of the gonads is not indicated in the initial evaluation. An abdominal radiograph does not help much in the initial diagnosis.
8.
(C)
Turner syndrome. Girls with Turner syndrome are usually born with normal female external and internal female genitalia but have streak ovaries as a result of accelerated ovarian atresia. Boys with Smith-Lemli-Opitz syndrome (a disorder of cholesterol biosynthesis caused by a deficiency of 7-dehydrocholesterol reductase) often present with hypospadias, a bifid scrotum, and cryptorchidism among other phenotypic abnormalities. Patients with Prader-Willi syndrome can present with micropenis in boys or hypoplasia of the labia majora in girls. They often have hypogonadism. Patients with trisomy 18 can have cryptorchidism and hypoplasia of the labia majora.
9.
(B)
Initiate testis formation. SRY is a transcription factor expressed in gonads with a Y chromosome, which is thought to initiate the molecular events of testis formation. Mutations within SRY have been associated with 46,XY sex reversal because of testicular failure.
10.
(B)
Converts testosterone into dihydrotestosterone. The enzymatic conversion of testosterone to dihydrotestosterone is critical for virilization of external male genitalia.
11.
(E)
All of the above. Expression of SRY is thought to be the initiating factor in testis formation. Thus deletion of SRY will cause sex reversal in 46,XY infants. 5-alpha-reductase is the enzyme that converts testosterone into the more biologically active dihydrotestosterone, and a deficiency results in undervirilization of male infants. Abnormality in the androgen receptor will cause undervirilization of males because of androgen insensitivity. 21-Hydroxylase deficiency blocks cortisol production, leading to androgen excess that causes overvirilization of female infants.
12.
(A)
Fallopian tubes, uterus, and upper vagina. In males, Müllerian-inhibiting hormone is secreted from the testicular Sertoli cells beginning at approximately the seventh week of gestation, and it causes regression of the Müllerian ducts.
13.
(E)
Epididymis, vas deferens, seminal vesicles. The Wolffian ducts differentiate into the epididymis, vas deferens, seminal vesicles, and ejaculatory ducts in 46,XY males.
14.
(B)
Produce testosterone that stabilizes the Wolffian ducts. Differentiation of the Wolffian ducts depends on local testosterone production from the Leydig cells of the testes.
15.
(E)
Dihydrotestosterone. Whereas development of the Wolffian ducts and internal genitalia depends on local production of testosterone, development of the external genitalia in males depends on dihydrotestosterone.
16.
(B)
46,XY, male internal genitalia, female external genitalia. 5-alpha-reductase deficiency is an autosomal recessive disorder in which 46,XY infants have bilateral testes and normal male internal genitalia (a result of normal testosterone production and production of Müllerian-inhibiting hormone that causes female internal genitalia to regress), but with undervirilized external genitalia because of defective conversion of testosterone to dihydrotestosterone. They typically present with microphallus, perineal hypospadias, and a blind vaginal pouch. At puberty, 46,XY patients undergo progressive virilization with phallic enlargement and muscular development because of testosterone production.
17.
(B)
Between 4 and 12 weeks’ gestation. The separation of the vagina and urethra is complete in females by 12 weeks. Exposure to excess androgens before this time can interfere with this process. Exposure to excess androgens once the vagina and urethra are separate causes clitoromegaly and rugation of the labial folds only. Formation of a urogenital sinus is common in virilized females with CAH.