Pediatric Examination and Board Review (105 page)
Read Pediatric Examination and Board Review Online
Authors: Robert Daum,Jason Canel

(A)
S pyogenes
(group A streptococci)
(B)
Streptococcus agalactiae
(C) group B streptococci
(D)
S aureus
(E) all of the above
6.
You see a 3-year-old girl who is brought to your office because of a lump in her neck that her parents noticed about 6 weeks prior. They are concerned that it is still present and not diminishing in size. In all other regards, the parents report she is in good health and has received all of her vaccinations. They live in a suburb and have no pets. They have not traveled in more than a year. On examination, she is afebrile and very cooperative. She has multiple firm, mobile left-sided cervical and submandibular nodes, the largest of which is 4.5 cm. There is no erythema, warmth, or drainage present. Her oral cavity, ears, conjunctivae, and scalp are normal. Her abdominal and skin examinations are normal.
Laboratory data include:
CBC: white blood count (WBC) 8.1 (48% lymphocytes, 33% neutrophils, 15% monocytes, 4% eosinophils)
ESR: 21
Purified protein derivative (PPD): 11 mm
What is the next test that should be ordered?
(A) blood culture
(B) chest radiograph
(C) lymph node biopsy
(D) CT of neck
(E) MRI of neck
7.
Which of the following is the most reliable way to ascertain the etiology of the infection in the patient in question 6?
(A) gastric lavage specimen
(B) sputum specimen
(C) urine specimen
(D) blood culture
(E) surgically excised tissue
8.
What is the least likely way that nontuberculous mycobacteria are transmitted?
(A) inhalation
(B) ingestion
(C) person to person
(D) direct contact with the organism
(E) animal contact
9.
Which of the following is the least likely clinical manifestation of the organism from a nontuberculous mycobacteria infection?
(A) skin ulcer
(B) disseminated infection
(C) bone infections
(D) lymphadenitis
(E) soft tissue infection
10.
The lymph node biopsy that you ordered grew
Mycobacterium intracellulare
, and the blood culture is negative. Which of the following is most likely to lead to a cure from question 6?
(A) ciprofloxacin
(B) doxycycline
(C) azithromycin and ethambutol
(D) azithromycin, ethambutol, and rifampin
(E) surgical excision
11.
You see a 4-year-old girl who comes in for a “lump” in her neck that she has had for about 3 weeks. Her parents do not recall any trauma to the area, toothaches, or illnesses in the last month. They are worried that she has “throat cancer” because her grandmother has just been diagnosed with the disease. She has 2 cats at home and has not traveled in the past 6 months. On examination you find a happy, cooperative child who is afebrile. She has a visible asymmetry of the neck. She has several leftsided tender cervical lymph nodes with overlying erythema and warmth. What is the most likely etiology of her disease?
(A)
Yersinia pestis
(B)
Francisella tularensis
(C)
Bartonella henselae
(D)
Chlamydia trachomatis
(E)
Corynebacterium diphtheriae
12.
Which of the following are other possible clinical manifestations of the organism from question 11?
(A) hepatitis
(B) aseptic meningitis
(C) Parinaud oculoglandular syndrome
(D) pharyngitis
(E) all of the above
13.
In which seasons is this disease most commonly manifested by the patient in question 11?
(A) winter/spring
(B) summer/fall
(C) summer/winter
(D) spring/fall
(E) no seasonal variance
14.
What is the best treatment for this patient from question 11?
(A) reassurance
(B) oral antibiotics
(C) get rid of cats in the home
(D) fine-needle aspiration
(E) incision and drainage
15.
You see a 5-year-old girl for a check-up and her parents tell you they are concerned about a small lump on her neck. It has been there for some time but was small and nontender, and they were waiting for their checkup to ask you about it. But 7 days ago she developed an upper respiratory tract infection with sneezing, coughing, and mild fever, and now the lump is larger than it was 2 weeks ago and somewhat tender. On examination you find a happy, cooperative, afebrile young girl. She has mild conjunctival injection bilaterally without discharge, red swollen turbinates and rhinorrhea, and a wet cough. Her lungs are clear. Her neck has a small 0.5-cm bulge in the midline, just above the suprasternal notch. It is tender to the touch and feels slightly boggy. There is no erythema. What is her most likely diagnosis?
(A) thyroid mass
(B) furuncle
(C) lymphadenitis
(D) thyroglossal duct cyst
(E) branchial cleft cyst
16.
Another 5-year-old girl is seen for a neck mass that also has been there for some time. She comes in because it is now tender and enlarging. Yesterday some “pus” started coming out of it. She has had no fever, had a “cold” 2 weeks ago, and is generally in good health. On examination she is afebrile. She has a 4-cm tender, smooth, fluctuant mass along the anterior border of the sternocleidomastoid muscle on the left side. There is a small dimple in the middle with yellow crust around it. You are able to express some serosanguineous fluid with mild pressure. The rest of her head and neck examination is normal. What is her diagnosis?
(A) thyroiditis
(B) furuncle
(C) lymphadenitis
(D) thyroglossal duct cyst
(E) branchial cleft cyst
17.
What is the best way to evaluate this lesion from question 16?
(A) radiograph of neck
(B) ultrasound of neck
(C) CT of neck
(D) MRI of neck
(E) B and C
18.
In regard to question 16, are these more often unilateral or bilateral?
(A) unilateral
(B) bilateral
ANSWERS
1.
(C)
This is most likely to be acute unilateral pyogenic lymphadenitis, often seen in children 1-4 years old following an upper respiratory tract infection. In more than 50% of cases, it is the submandibular nodes that are affected. The tempo of the illness and the overlying illness are the most important clues. Cat-scratch disease is a possibility but less likely.
2.
(D)
EBV usually causes either bilateral or generalized lymphadenopathy and more constitutional symptoms. Group A streptococci and
S aureus
cause more than 80% of cases like these. Infections caused by nontuberculous mycobacteria more often have an insidious onset, although they can uncommonly cause a picture similar to acute pyogenic lymphadenitis.
3.
(D)
Because staphylococci and streptococci are the primary pathogens, an oral cephalosporin such as cephalexin is the most appropriate choice in areas where the prevalence of MRSA in the community is low. Clindamycin would be a better choice if community-acquired MRSA is common in the patient’s area.
4.
(E)
5.
(E)
S aureus
is the most common cause of neonatal acute cervical lymphadenitis, but another important cause of neck mass in the newborn is group B streptococci, the “cellulitis-adenitis” syndrome. This most often presents at 3-7 weeks, 75% of patients are boys, and most have the overlying cellulitis previously described.
S agalactiae
and group B streptococci are synonyms.
6.
(B)
It is essential to exclude
M tuberculosis
as early as possible because of the abnormal PPD (a positive tuberculin skin test in an otherwise healthy 3-yearold is >10 mm). However, caution must be used in interpreting PPD results in children in whom a nontuberculous mycobacterial (NTM) infection is possible because antigens of the latter can elicit a response with PPD. A chest radiograph should be the next test ordered. After that, a lymph node biopsy and a CT scan of the neck are possible further avenues of investigation.
7.
(E)
Because NTM are present in the environment (soil, water), specimens from nonsterile locations such as stomach, urine, and sputum can be contaminated. A blood culture will only be positive if disseminated disease is present, a rare event. Examination and culture of the tissue obtained by surgical excision is the gold standard to diagnose caseating granulomatous infections in the presence of an 11 mm PPD.
8.
(C)
NTM are found in soil and water, and transmission can be by inhalation, ingestion, direct contact, and animal contact by means of soil and water. Person-to-person transmission is rare.
9.
(B)
NTM can cause the other infections listed, but disseminated infection occurs only in immunocompromised hosts. Children with CF may have NTM in their sputum.
10.
(E)
For NTM in an otherwise healthy child, complete surgical excision almost always leads to cure. Ciprofloxacin and doxycycline may be effective against rapidly growing mycobacteria (
M fortuitum, M abscessus
). C and D represent multidrug therapy, reserved for immunocompromised patients or those with disseminated disease. Ethambutol is seldom used in children.
11.
(C)
This is most likely cat-scratch disease caused by
Bartonella henselae
, although the patient is afebrile. In more than three-fourths of cases, a history of a cat or kitten exposure is given (see
Figure 64-1
).
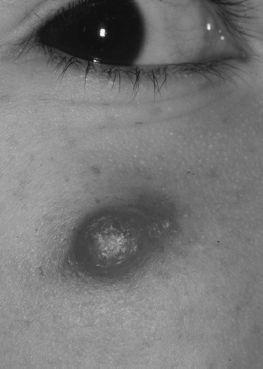
FIGURE 64-1.
Bartonellosis: cat-scratch disease with primary lesion. Erythematous nodule of the cheek of a 9-year-old girl at the site of the cat scratch. Diagnosis was made on the histologic findings of the excised specimen. (Reproduced, with permission, from Wolff K, Johnson RA. Fitzpatrick’s Color Atlas & Synopsis of Clinical Dermatology, 6th ed. New York: McGraw-Hill; 2009: Fig. 24-55.)