Oxford Handbook of Midwifery (100 page)
Read Oxford Handbook of Midwifery Online
Authors: Janet Medforth,Sue Battersby,Maggie Evans,Beverley Marsh,Angela Walker

- R = REMOVE POSTERIOR ARM, midwife’s hand enters posteriorly along arm, flexes arm and grasps hand, sweeping the baby’s arm across his chest and face to deliver.
Consider other options;
- Place mother in all fours position: change of position may dislodge the anterior shoulder, may facilitate access for internal manoeuvres.
- Fracture clavicle, symphysiotomy (division of symphysis), and Zavanelli manoeuvre (cephalic replacement and delivery by caesarean). (The last three options would need to be performed by an obstetrician. They are last resort measures.)
Document the head to body delivery interval, order of manoeuvres, and cord pH.
Debrief—full and clear explanations should be given to the parents. The professionals involved should be offered the chance to discuss the case in a supportive environment.
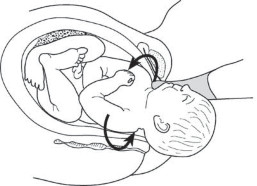
Fig. 19.7
Wood’s screw manoeuvre. Rotate anterior shoulder.Reprinted by permission of Henry Lerner M.D. from M
www.shoulderdystociainfo.com.
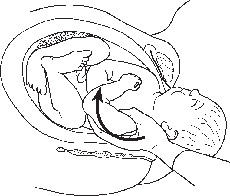
Fig. 19.8
Rubin’s manoeuvre. Rotate posterior shoulder.Reprinted by permission of Henry Lerner M.D. from M
www.shoulderdystociainfo.com.SHOULDER DYSTOCIA
449
1
The Confidential Enquiry into Stillbirths and Neonatal Deaths. 5th Annual Report. London: CESDI, pp. 73–9. Available at: M
www.cesdi.org.uk (accessed 25.2.11).
CHAPTER 19
Emergencies450
Guidelines for admission to neonatal ICU
‘Provision for sick neonates has developed rapidly over the last two decades from a small area on a maternity ward to a giant, technical, scientifically based system of care. Advances in technology and an increased understanding of the problems and needs of premature and low birth weight babies have increased the survival rates of babies who would have died a few years ago
.’
1
In 1992 the WHO
2
clarified the definitions for premature and small fordate babies:
- A
premature baby
is any baby born before 37 completed weeks of gestation. - A
small for date baby
is a baby whose weight falls below the 10th percentile for its gestational age.These definitions indicate that a baby can be both premature and small for dates, or term and small for dates.
- About 6.7% of babies born in the UK will weigh <2.5kg.
- One-third will be small for dates; 70% will weigh between 2kg and 2.5kg.
- About 50% of those weighing 1.5–2kg will have minimal or no illness in the neonatal period.
- A
term baby
is one born between 37 and 42 weeks’ gestation, with an average weight of 3.5kg on the 50th percentile. - A baby can be
large for dates
, with a weight of 4.5kg or more at birth, which is on the 90th percentile. This can be normal, but is also associated with maternal diabetes.
In 1990 the Human Fertilization and Embryology Act stated that a baby is capable of surviving from 24 weeks of pregnancy. Viable gestational age is considered by law to be 24 weeks, whatever the baby’s weight.
1,3The current structure of neonatal care in the UK
Regional units
Full intensive expert care is provided for the smallest, sickest babies. There is also provision for neonatal surgery. Mothers are referred to these centres for delivery if problems are indicated, or retrieval teams will collect the baby following delivery and stabilization. It is preferable to transfer the baby
in utero
as, once born, its survival depends on provision of a stable thermal environment and effective management of oxygena- tion. Transferring a small, sick baby in the back of an ambulance can prove to be very hazardous. The baby returns to the referring unit once he or she is well enough.Subregional units
These are subsidiary to the regional units. They provide full expert inten- sive care. The only difference being that they do not provide surgery, and will transfer any baby requiring surgery to the nearest surgical unit.
Special care baby units
These are based in all maternity hospitals, for the care of small babies from 32 weeks’ gestation. They can also provide emergency treatment and stabilization for the smaller, sicker babies, until transfer to the regional

GUIDELINES FOR ADMISSION TO NEONATAL ICU
451
unit can be arranged. They usually have two or three intensive cots and may keep the baby if it can be managed within that context.
Transitional care units
These are usually based on a maternity ward away from the intensive and high-dependency care contexts, thus keeping the baby with or near to its mother, and cared for by midwives or neonatal nurses. Babies needing this level of care usually require treatment for jaundice or infections, or they may be small but are otherwise well.
Criteria for admission to the NICU
4 - A
- Place mother in all fours position: change of position may dislodge the anterior shoulder, may facilitate access for internal manoeuvres.
- R = REMOVE POSTERIOR ARM, midwife’s hand enters posteriorly along arm, flexes arm and grasps hand, sweeping the baby’s arm across his chest and face to deliver.
- Any baby weighing <1700g from 23–34 weeks’ gestation.
- Any baby who is ill at birth; for example, extremely small for dates.
Other books
Death in the Jungle by Gary Smith
The Crisis of Islam: Holy War and Unholy Terror by Bernard Lewis
A Cool Breeze on the Underground by Don Winslow
Nil Unlocked by Lynne Matson
The Irish Upstart by Shirley Kennedy
The Way We Were by Kathryn Shay
The Bandit King by Saintcrow, Lilith
A Sticky Situation by Jessie Crockett
The Silence of Bonaventure Arrow by Rita Leganski
The Enemy Within (Daughters of the People Series Book 3) by Varna, Lucy