In Search of Memory: The Emergence of a New Science of Mind (17 page)
Read In Search of Memory: The Emergence of a New Science of Mind Online
Authors: Eric R. Kandel
Tags: #Psychology, #Cognitive Psychology & Cognition, #Cognitive Psychology

In 1879 Carl Wernicke (figure 8–2) described a second type of aphasia. This disorder is not an impairment in the production of speech, but a disruption in the comprehension of spoken or written language. Moreover, while people with Wernicke’s aphasia can speak, what they say is completely incoherent to anyone else. Like Broca’s aphasia, this aphasia is caused by a lesion in the left side of the brain, but in this case the damage is in the back of the brain, in a region now called Wernicke’s area (figure 8–2).
Based on his own and Broca’s work, Wernicke put forward a theory of how the cortex is wired for language. That theory, although simpler than our current understanding of language, is nevertheless consistent with how we view the brain today. As a first principle, Wernicke proposed that any complex behavior is the product not of a single region but of several specialized, interconnected areas of the brain. For language, these are Wernicke’s area (comprehension) and Broca’s area (expression). The two areas, as Wernicke knew, are connected by a neural pathway (figure 8–3). He also understood that large, interconnected networks of specialized regions, such as those governing language, enable people to experience mental activity as seamless.
The idea that different regions of the brain are specialized for different purposes is central to modern brain science, and Wernicke’s model of a network of interconnected, specialized regions is a dominant theme in the study of the brain. One reason this conclusion eluded investigators for so many years can be found in another organizational principle of the nervous system: brain circuitry has a built-in redundancy. Many sensory, motor, and cognitive functions are served by more than one neural pathway—the same information is processed simultaneously and in parallel in different regions of the brain. When one region or pathway is damaged, others may be able to compensate, at least partially, for the loss. When compensation occurs and no behavioral deficits are obvious, researchers have difficulty linking a damaged site in the brain to a behavior.
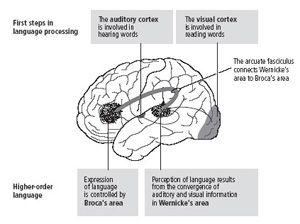
8–3
Complex behavior, such as language, involves several interconnected areas of the brain.
Once it was known that language is produced and understood in specific regions of the brain, regions governing each of the senses were identified, providing a foundation for Wade Marshall’s later discoveries of sensory maps for touch, vision, and hearing. It was only a matter of time before these searches turned to memory. Indeed, the fundamental question of whether memory is a unique neural process or is associated with motor and sensory processes remained open.
INITIAL ATTEMPTS TO PINPOINT A REGION OF THE BRAIN
responsible for memory, or even to delineate memory as a unique mental process, failed. In a series of famous experiments in the 1920s, Karl Lashley trained rats to run through a simple maze. He then removed different areas of the cerebral cortex and retested the rats twenty days later to see how much training they had retained. Based on these experiments, Lashley formulated the law of mass action, which holds that the severity of memory impairment is correlated with the size of the cortical area removed, not with its specific location. Thus Lashley wrote, echoing Flourens a century earlier, “It is certain that the maze habit, when formed, is not localized in any single area of the cerebrum [the cerebral cortex] and that its performance is somehow conditioned by the quantity of tissue which is intact.”
Many years later Lashley’s results were reinterpreted by Wilder Penfield and Brenda Milner at the Montreal Neurological Institute. As more scientists experimented with rats, it became clear that mazes were not suitable for studying the location of memory function. Maze learning is an activity that involves many different sensory and motor capabilities. When an animal is deprived of one kind of sensory cue (for example, touch), it can still recognize a place reasonably well using other senses (such as vision or smell). In addition, Lashley focused his efforts on the cerebral cortex, the outer layer of the brain; he did not explore the structures that lie deeper in the brain. Subsequent research has shown that many forms of memory require one or more of these deeper regions.
The first suggestion that some aspects of human memory can be stored in specific regions of the brain arose in 1948 from Penfield’s neurosurgical work (figure 8–4). Penfield had trained in physiology with Charles Sherrington while on a Rhodes scholarship. He began to use surgery to treat focal epilepsy, a disorder that produces seizures in limited regions of the cortex. He developed a technique, still used today, of removing epileptic tissue while avoiding or minimizing damage to areas involved in the patient’s mental processes.
Because the brain contains no pain receptors, surgery can be carried out with a local anesthetic. Thus Penfield’s patients remained fully conscious during surgery and were able to report their experiences. (In describing this to Sherrington, who had spent his career working on cats and monkeys, Penfield could not resist adding, “Imagine having an experimental preparation that can talk back to you.”) Penfield applied weak electrical stimulation to various areas of his patients’ cerebral cortex during surgery and determined the effects of this stimulation on their ability to speak and comprehend language. Through his patients’ responses, he could pinpoint Broca’s and Wernicke’s areas and try to avoid damage to them when removing epileptic tissue.

8–4
Wilder Penfield (1891–1976) exposed the surface of the brain in conscious patients during surgery for epilepsy. He then stimulated different parts of the cortex and through the patients’ responses identified the temporal lobe as a potential site for memory storage. (Courtesy of the Penfield Archive and the Montreal Neurological Institute.)
Over the years, Penfield explored much of the surface of the cerebral cortex in more than a thousand persons. On occasion, in response to electrical stimulation, a patient would describe complex perceptions or experiences: “It sounded like a voice saying words, but it was so faint that I couldn’t get it.” Or, “I am seeing a picture of a dog and cat…the dog is chasing the cat.” Such responses were rare (occurring in only about 8 percent of cases) and were invariably elicited only from the temporal lobes of the brain, never from other areas. The responses suggested to Penfield that the experiences elicited by electrical stimulation of the temporal lobes are snippets of memory, of the stream of experience in a person’s life.
Lawrence Kubie, the psychoanalyst whom I knew through Ernst Kris, traveled to Montreal and used a tape recorder to monitor Penfield’s patients’ utterances. Kubie became convinced that the temporal lobe stored a particular type of unconscious information called the preconscious unconscious. I read an important paper by Kubie when I was in medical school and heard him lecture several times while I was working in Grundfest’s lab, and I was influenced by his enthusiasm for the temporal lobe.
In time, Penfield’s view that the temporal lobes store memory was called into question. First, all of his patients had abnormal brains because of their epilepsy; moreover, in almost half of the cases the mental experience evoked by stimulation was identical to the hallucinatory mental experiences that often accompanied seizures. These findings convinced most brain scientists that Penfield was eliciting seizurelike phenomena with his electrical stimulation—specifically, that he might be eliciting the auras (hallucinatory experiences) characteristic of the early phase of an epileptic attack. Second, the reports of mental experiences included elements of fantasy as well as improbable or impossible situations; they were more like dreams than memories. Finally, removing the brain tissue under the stimulating electrode did not erase the patient’s memory.
Nevertheless, a number of neurosurgeons were inspired by Penfield’s work, among them William Scoville, who obtained direct evidence that the temporal lobes are critical to human memory. In the paper that I had read on arriving at NIH, Scoville and Brenda Milner reported the extraordinary story of a patient known to science only by his initials, H.M.
AT THE AGE OF NINE, H.M. WAS KNOCKED DOWN BY SOMEONE
riding a bicycle. He sustained a head injury that led eventually to epilepsy. Over the years, his seizures worsened, until he was having as many as ten blackouts and one major seizure a week. By age twenty-seven, he was severely incapacitated.
Because H.M.’s epilepsy was thought to have originated within the temporal lobe (specifically, the medial temporal lobe), Scoville decided, as a last resort, to remove the inner surface of that lobe on both sides of the brain, as well as the hippocampus, which lies deep within the temporal lobe. The surgery succeeded in relieving H.M.’s seizures, but it left him with a devastating memory loss from which he never recovered. After his operation in 1953, H.M. remained the same intelligent, kind, and amusing man he had always been, but he was unable to convert any new memories into permanent memory.
In a series of studies, Milner (figure 8–5) documented in exquisite detail the memory ability H.M. had lost, the memory ability he retained, and the areas of the brain responsible for each. She found that what H.M. retained was remarkably specific. To begin with, he had perfectly good short-term memory, lasting for minutes. He could readily remember a multidigit number or a visual image for a short period after learning it, and he could carry on a normal conversation, provided it did not last too long or move among too many topics. This short-term memory function was later called working memory and shown to involve an area known as the prefrontal cortex, which had not been removed from H.M. Second, H.M. had perfectly good long-term memory for events that had occurred before his surgery. He could remember the English language, his IQ was good, and he recalled vividly many events from his childhood.

8–5
Brenda Milner (b. 1918), whose studies of H.M. opened up the modern study of memory storage by localizing memory to a particular site in the brain. Milner identified the roles of the hippocampus and the medial temporal lobe in explicit memory and provided the first evidence of implicit memory storage. (Reprinted from
Essentials of Neural Science and Behavior
, Kandel, Schwartz, and Jessell, McGraw-Hill, 1995.)
What H.M. lacked, and lacked to the most profound degree, was the ability to convert new short-term memory into new long-term memory. Without this ability he forgot events shortly after they happened. He could retain new information as long as his attention was not diverted from it, but a minute or two after his attention was directed to something else, he could not remember the previous subject or anything he thought about it. Less than an hour after eating he could not remember anything he had eaten or even the fact that he had had a meal. Brenda Milner studied H.M. monthly for almost thirty years, and each time she entered the room and greeted him he failed to recognize her. He did not recognize himself in recent photographs or in the mirror because he remembered himself only as he was prior to surgery. He had no memory of his changed appearance: his identity has been frozen for over fifty years, from the time of his surgery until today. Milner was to say of H.M., “He couldn’t acquire the slightest new piece of knowledge. He lives today chained to the past, in a sort of childlike world. You can say his personal history stopped with the operation.”