Resident Readiness General Surgery (10 page)
Read Resident Readiness General Surgery Online
Authors: Debra Klamen,Brian George,Alden Harken,Debra Darosa
Tags: #Medical, #Surgery, #General, #Test Preparation & Review

The primary survey is best accomplished in a team-oriented, standardized fashion in order to ensure the best possible outcome for the patient. The mnemonic ABCDE (
A
irway,
B
reathing,
C
irculation,
D
isability, and
E
xposure/
E
nvironment) is useful in helping one remember the order in which the primary
survey should be carried out. Note that these steps should be repeated any time there is a change in the patient’s status.
The first priority should always be the
a
irway, with the assessment focused on determining if the patient’s airway is patent or not and, if so, determining whether or not the patient can maintain an intact airway. This can be initially assessed by simply asking the patient a question such as “What is your name?” If the patient is able to speak in a clear voice, the airway is intact. However, if there is no response, speech is garbled, or it takes considerable effort to speak, intervention is required. This may simply consist of a chin lift, jaw thrust maneuver to open up the airway, suctioning if the airway is occluded by blood or vomitus, or removal of any foreign bodies. In some cases, however, placement of an endotracheal tube (ETT) is indicated. If orotracheal or nasotracheal intubation is not possible, then a surgical airway (ie, cricothyroidotomy) may be necessary. During the airway assessment, inline stabilization of the cervical spine should be maintained until a cervical injury has been ruled out.
Next, the patient’s breathing or the ability to ventilate should be assessed. An inspection of the chest and neck may identify the presence of penetrating injuries, bruising, tracheal deviation (ie, from a tension pneumothorax), and abnormal chest wall movements (ie, from a flail chest). Auscultation may reveal the absence of breath sounds or asymmetry (ie, as a result of a pneumothorax). Life-threatening injuries to the chest should be addressed at this point prior to moving on with the remainder of the survey. This is particularly the case if the patient has a suspected tension pneumothorax, in which treatment entails immediate needle decompression followed by tube thoracostomy placement.
The patient’s circulation should then be evaluated as hemorrhage is the most common cause of preventable postinjury deaths. This is assessed by looking for any evidence of external hemorrhage, palpating central pulses (most commonly the carotids or femorals), obtaining a blood pressure and heart rate, and taking note of any distended neck veins or muffled heart sounds (both of which are highly concerning for cardiac tamponade). Any external bleeding should be controlled by applying direct pressure. Cardiac tamponade should be treated immediately by a pericardiocentesis or pericardial window. In general, hypovolemia should be treated with aggressive fluid resuscitation after the establishment of 2 large-bore (14- or 16-gauge) IV catheters.
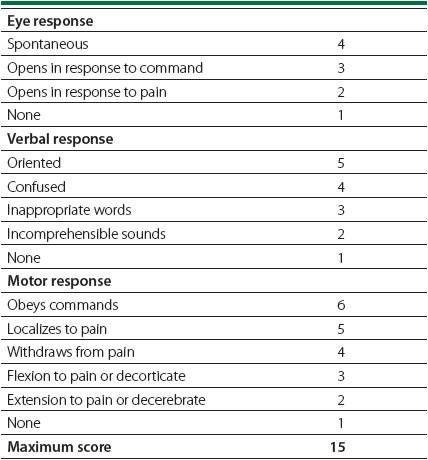
The disability of a patient can be determined by performing a quick evaluation of the pupils and by making an assessment of mental status and gross motor function in all 4 extremities. Examine the pupils for any discrepancies in size, symmetry, and reactiveness to light. Use the Glasgow Coma Scale (GCS) to quantify the degree of neurologic abnormalities and to determine if the level warrants emergent intubation (ie, if the GCS is less than 8; see
Table 7-2
).
Table 7-2.
Glasgow Coma Scale
Finally, the patient’s body should be completely exposed by removing all clothing. This facilitates the full head-to-toe examination that should be carried out during the secondary survey in order to look for any previously missed injuries. At this time, the patient’s back should also be examined for any signs of spinal injury in the form of tenderness or bony step-offs, and the axillae and perineum evaluated for any traumatic wounds. Be sure to cover the patient with warm blankets and be sure to maintain cervical spine stabilization when logrolling the patient to assess the back.
TIPS TO REMEMBER
The goal of the trauma primary survey is to identify and treat any life-threatening injuries.
COMPREHENSION QUESTIONS
1.
While in the midst of exposing the patient during the primary survey, one of the ED nurses announces that the patient’s SBP has dropped from 120 mm Hg on arrival to 70 mm Hg. The trauma team leader orders the initiation of a 2 L fluid bolus. In addition to this, the next step should be which of the following?
A. Pericardiocentesis as you weren’t sure if the heart sounds were normal during the initial assessment.
B. Take the patient to the CT scanner to determine the source of the hypotension.
C. Repeat the steps of the primary survey, starting with a reassessment of the patient’s airway.
D. Proceed with the secondary survey.
2.
A patient is brought to the trauma bay after sustaining a fall from the roof of his 2-story home. When a deep sternal rub is applied to the patient, he extends his arms and legs. He lacks any eye or verbal response. What is the patient’s GCS score?
A. 4
B. 8
C. 9
D. 12
3.
Which scenario meets criteria for trauma team activation?
A. A patient who “twists” her ankle after falling from a chair in her kitchen.
B. A patient who was hit by an oncoming car driving at a speed of 25 mph.
C. A patient who is rear-ended in a parking garage by a car driving at speed of 10 mph.
D. None of these scenarios meet criteria for trauma team activation.
Answers
1.
C
. With any change in a patient’s status, you should quickly repeat the ABCDEs of the primary survey before moving on with the rest of the assessment (secondary survey). It was okay for the trauma team leader to order a fluid bolus as this can be done concurrently with the primary survey. Pericardiocentesis is seldom performed without a high index of suspicion, such as a positive FAST or high-risk mechanism, like a stab wound to the chest. Even then it is used only as an
emergent bridge to definitive therapy, which would be thoracotomy or sternotomy with cardiac repair. Finally, the patient in this scenario is too unstable to undergo a CT scan. Furthermore, determining the source of the patient’s hypotension may not require the use of CT imaging.
2.
A
. The absence of eye (1) or verbal responses (1) paired with decerebrate posturing (2) would give the patient a GCS score of 4.
3.
B
. This scenario meets criteria for trauma team activation because of the speed of >20 mph.
 A 40-year-old Female With Abdominal Pain
A 40-year-old Female With Abdominal Pain
Other books
Horse Play (Horse Play #1) by A. D. Ryan
March With Venus: 94 Love Games (Book 7) by Peters, Karma
Milkweed Ladies by Louise McNeill
Witches and Whatnots: An Izzy Cooper Novel by Kendra Ashe
Road to Recovery by Natalie Ann
Will to Love by Miranda P. Charles
Summer Boys by Hailey Abbott
Time Commander (The First Admiral Series) by Benning, William J.
Needing by Sarah Masters
Lycan Fallout: Rise Of The Werewolf by Tufo, Mark