Women's Bodies, Women's Wisdom (89 page)
Read Women's Bodies, Women's Wisdom Online
Authors: Christiane Northrup
Tags: #Health; Fitness & Dieting, #Women's Health, #General, #Personal Health, #Professional & Technical, #Medical eBooks, #Specialties, #Obstetrics & Gynecology

Fertility awareness techniques (with or without barrier contraceptives during ovulation) can be highly effective means of birth control. The Ovulation Method has been studied most rigorously at Creighton University in Omaha, Nebraska. Three major studies show that the effectiveness of the method for avoiding pregnancy can be 99.1 to 99.9 percent, while actual user rates ranged from 94.8 to 97.3 percent. The differences in these figures were attributable to teaching-and use-related errors.
26
Fertility awareness techniques that let you know when you ovulate also can enhance chances of conception considerably. It is generally accepted that the probability of conceiving in one cycle for couples with normal fertility is in the range of 22 to 30 percent. But in one study of couples using fertility-focused intercourse, 71.4 percent of the clients who had a previous pregnancy achieved pregnancy in the first cycle. With those clients who had never had a pregnancy, the rate was 80.9 percent. By the fourth cycle, 100 percent of those who had never been pregnant had conceived.
27
In couples who are having difficulty conceiving, using the Ovulation Method alone without any other testing can considerably enhance the chances of conception. Dr. Stanford notes that “of cou ples referred to the NFP [natural family planning] center at Omaha for inability to achieve pregnancy [for an average of three years], 20 to 40 percent have achieved pregnancy within six months of use of the Ovulation Method, before any further medical evaluation and treatment is undertaken.”
28
The Ovulation Method also works well for those who have irregular periods, are breastfeeding, or are perimenopausal.
I strongly recommend the Ovulation Method to any committed couple. Dr. Stanford, like other experts in fertility aware ness, always refers patients to a thoroughly trained natural family planning counselor, because although the method is simple, it requires support and education, especially in the beginning. Obviously, introducing fertility con sciousness into the whole area of sexuality and working with it daily is a pretty new concept for many. Adequate personalized instruction by qualified teachers is essential for the successful use of natural family planning in general and the Ovulation Method in particular. It is not learned well from a book, most likely because of the emotional and psychological issues it brings up. The quality of a woman’s (or couple’s) experience with this method often depends upon the quality of instruction given and follow-up care received.
Couples who use fertility awareness effectively throughout their reproductive lives experience no side effects and often find an increased intimacy in their relationships, which includes a shared responsibility for their combined fertility. Though we tend to associate interest in natural family planning with certain religions, many women are drawn to this method because it is, inherently, a holistic approach to fertility. I suspect that if this method was more widely known and supported by health care professionals, it would be more widely used. Whether or not you use fertility awareness for contraceptive or conception purposes, it is empowering to know your fertility cycle. Here’s a brief overview of the method.
Defining the fertile phase.
The egg lives anywhere from six to twenty-four hours after ovulation. But sperm can live for up to five days in fertile mucus, which means that sperm deposited up to five days before ovulation actually occurs can cause a pregnancy. (Without fertile mucus, they die in a few hours.) Therefore, there is about a seven-day time period during every cycle when pregnancy is at least theoretically possible. One study found that among healthy women trying to conceive, nearly all pregnancies could be attributed to intercourse during a six-day period ending on the day of ovulation. Though no one in the study conceived on the day after ovulation, the authors of the study concluded that there was probably a 12 percent chance of conceiving on the day after ovulation and also on the sev enth day before ovulation. The study also concluded that for those couples trying to conceive, having intercourse every other day was just as effective as every day. Practically speaking, if you are trying to get pregnant, have intercourse four times during your most fertile week. This is usually more effective, and less stressful, than trying to stick to an every-other-day schedule.
29
It has been my experience, however, that despite the best information science has to offer, sometimes when a soul is meant to come in, it will—no matter what you do or don’t do.
Mucus checks (natural birth control).
Studies have shown that almost all women can easily learn to check for the presence or absence of fer tile E-type (estrogen-stimulated) mucus by the routine observation of vaginal discharge on the vulva.
30
As menstruation stops, cervical mucus is at a minimum. You feel dry. There is no mucus in the vaginal opening and no discharge on your underwear. This lack of mucus is associated with being infertile. These “dry” days are usually safe for unprotected intercourse. The cervix begins secreting E-type mucus about six days prior to ovulation, so, using this method, you will know when ovulation is apt to occur before it happens. When you see mucus on your underwear or can wipe it off with toilet paper, you know your fertile time is beginning. E-type mucus, when looked at under the microscope, contains channels that help the sperm swim up through the cervix. It also dries into a characteristic ferning pattern. Fertile mucus is similar in feel and quality to uncooked egg white. Some women may even notice that it wets their underwear. You are fertile from the time when fertile mucus first appears until the fourth day after your peak mucus discharge. The last day of any mucus that is clear, stretchy (greater than or equal to one inch of stretch between thumb and index finger), or lubricative is called the peak day of mucus discharge. This peak mucus day is highly correlated with ovulation, which occurs plus or minus two days from this peak day more than 95 percent of the time.
31
G-type mucus (progesterone-stimulated) appears immediately after ovulation. This type of mucus lacks elasticity. It also has an opaque and adhesive quality. G-type mucus, when looked at under the microscope, lacks the channels that facilitate the swimming of sperm. This type of mucus actually blocks the passage of sperm. Following ovulatory mucus discharge, cervical mucus may cease (you become dry) or become thicker and more dense (G-type mucus). Either way, the change is distinct and noticeable. Your period will start about twelve to fifteen days after the peak ovulatory cervical flow.
32
As already mentioned, saliva also changes cyclically with your hormonal cycle. As your hormones change during your cycle, your saliva, when dry, develops a special microscopic ferning pattern that matches that of the cervical mucus. Special small microscopes are available and widely used in Europe and Japan as yet another way for women to learn about and therefore make the best use of their fertility cycle, whether the goal is to conceive or avoid pregnancy.
Keep a record of your basal body temperatures for three months to seeif you are ovulating.
Though learning how to assess your cervical mucus is also accurate, taking your basal body temperature and recording it for a few cycles is an empowering way to learn about your body and its internal rhythms. It also enhances your ability to correlate your cervical mucus and/or salivary changes with ovu lation.
The temperature rise that occurs with ovulation is due to the effect of progesterone. If you become pregnant during the period in which you have been taking your basal body temperature, you will notice that it stays up and doesn’t drop down again. This tempera ture elevation on BBT is a very early sign of pregnancy. (When women are pregnant, they have a great deal of progesterone in their systems and their temperature is higher than in the non-pregnant state. Pregnancy was the only time I could comfortably swim in the ocean in Maine.)
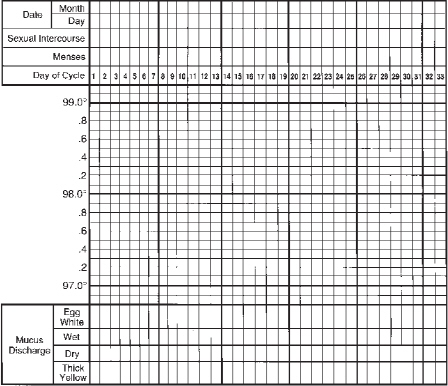
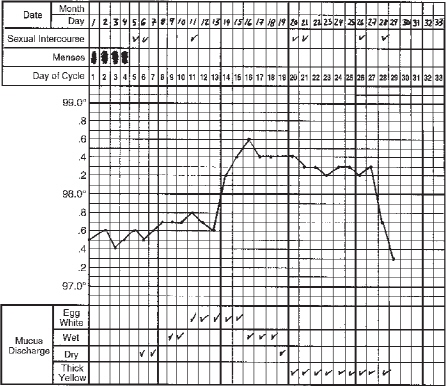
Take your basal body temperature first thing each morning starting on the first day of your menstrual period. (This is considered day one of your cycle.) Do this for three cycles, and chart each cycle sep arately. You can then use your temperature graph to record cervical mucus and salivary changes. (see
figure 15
.) Ovulation is accompa nied by a rise in basal body temperature of about 0.6 to 0.8 degrees, and it occurs somewhere between the time when the temperature begins to rise and the time when it reaches its highest point. The fertile time generally is over at the end of the third day in a row of elevated temperature. (see
figure 15
.)
FIGURE 15: FERTILITY AWARENESS:
OVULATION AND BASAL BODY TEMPERATURE
If your cycles are quite regular, you can get a general idea of the length of your fertile and infertile times by charting the following: Record cycle length for at least six months to determine the earliest possible day that your ovulation could occur. The follicular phase of the cycle (from day one of your period until ovulation) is variable in length. The luteal phase (the time from ovulation to onset of your period) is generally fixed at fourteen days. To determine the earliest day of the cycle when you could ovulate, subtract fourteen from your shortest cycle length. Therefore, if your cycle ranges in length from twenty-six to thirty-one days, the earliest you could ovulate is day twelve (26 - 14 = 12). Depending upon your cervical mucus, you could probably have intercourse until day eight or nine of your cycle and avoid pregnancy. (In doing these calculations, you can easily see why charting mucus flow or salivary ferning patterns is generally more accurate than this “calendar” method.)
FIGURE 15: FERTILITY AWARENESS:
OVULATION AND BASAL BODY TEMPERATURE
Permanent Contraception
Tubal Ligation
Tubal ligation is the most common form of permanent contraception in the United States. Many women are ambivalent about it, how ever, even when they know intellectually they don’t want more children. Most of us value the
ability
to conceive, even if we choose not to use that ability. Permanent contraception closes a door that usually cannot be reopened. For centuries, women were valued solely for their ability to bear children, and bearing children has been the most important socially acceptable outlet for women’s creative power. Voluntarily giving up this capacity stirs primitive fears. Yet many women find that being free of the fear of pregnancy is health-enhancing and rejuvenates their sexuality.
Tubal ligation is an excellent choice for some women—but not all. I chose this procedure after waiting until my younger daughter was four. Somehow, though there is no logic to it, this made me feel that she was “safe” and “permanent.” At about the age of thirty-seven, my path was split in front of me in terms of childbearing. I knew that having another child would mean at least another five years of energy diverted to the needs of the child and away from my own pursuits. I still went mushy sometimes looking at babies in air ports, and I harbored a secret fantasy of having the ideal pregnancy and the ideal labor, in which I would rest and really enjoy the pregnancy
and
the new baby—things I had not done fully with my other two children.
But I had seen far too many women become pregnant “accidentally” in their late thirties and early forties, just as their lives were settling down after a decade or so devoted to the demands of raising children. I was at a point where I had to make a conscious choice one way or the other about having another child. I wouldn’t have had an abortion if I became pregnant at this time in my life. (If I had become pregnant during my training years, however, I would have had an abortion without hesitation.) Still, I didn’t want a pregnancy just to happen. I wanted to be a conscious decision maker, not have my life decided by “fate.”