Wallach's Interpretation of Diagnostic Tests: Pathways to Arriving at a Clinical Diagnosis (543 page)
Authors: Mary A. Williamson Mt(ascp) Phd,L. Michael Snyder Md

BOOK: Wallach's Interpretation of Diagnostic Tests: Pathways to Arriving at a Clinical Diagnosis
9.05Mb size Format: txt, pdf, ePub
Focal nephritic: generally associated with inflammatory regions in less than one half of glomeruli. Patients often present with asymptomatic hematuria and proteinuria.
Causes
Renal: can be postinfectious (due to certain nephritogenic strains after streptococcal, staphylococcal, or pneumococcal infections, mumps, measles, chickenpox, hepatitis B and C) or due to MPGN or anti–glomerular membrane disease.
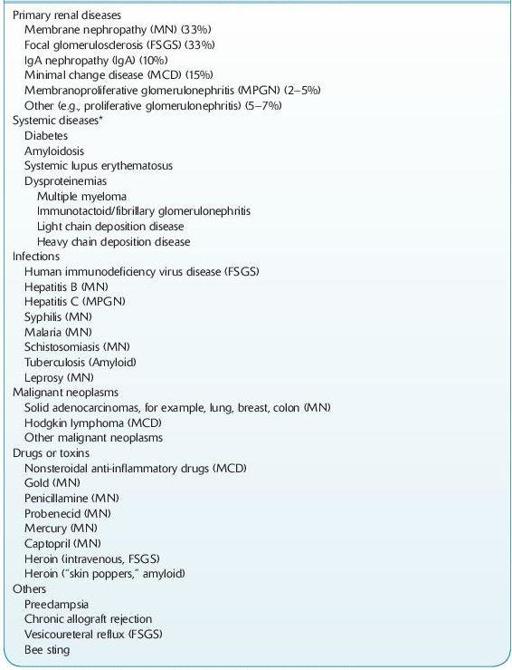
NEPHROTIC SYNDROME
This syndrome presents as heavy proteinuria, hypoalbuminemia, hyperlipidemia, lipiduria, and edema.
12-5
).
TABLE 12–5. Major causes of Nephrotic Syndrome
Other books
Mañana lo dejo by Gilles Legardinier
Protector of the Pride (Lions of Pride Island Book 3) by Terry Bolryder
No Rules by R. A. Spratt
Last Call (Stranded in the Stars Book 1) by Naomi Lucas
Redefined by Jamie Magee
The Lord of the Rings by J. R. R. Tolkien
Ann Veronica by H. G. Wells
Physical by Gabriella Luciano
Wetware by Craig Nova
Valentine Present and Other Diabolical Liberties by Lynda Renham