Wallach's Interpretation of Diagnostic Tests: Pathways to Arriving at a Clinical Diagnosis (525 page)
Authors: Mary A. Williamson Mt(ascp) Phd,L. Michael Snyder Md

The majority of CKD cases are due to glomerular disease, tubular or interstitial disease, or long-standing obstructive uropathy.
TABLE 12–3. Classification and Clinical Action Plan for Chronic Kidney Disease
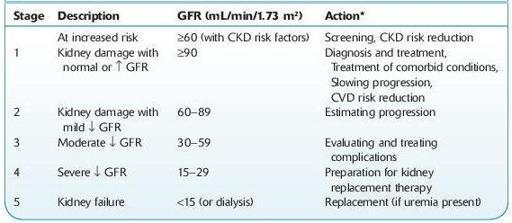
Shaded area identifies patients who have chronic kidney disease; unshaded area designates individuals who are at increased risk for developing chronic kidney disease.
*Includes actions from preceding stages.
GFR, glomerular filtration rate; CKD, chronic kidney disease; CVD, cardiovascular disease.
Source: National Kidney Foundation. K/DOQI clinical practice guidelines for chronic kidney disease: evaluation, classification and stratification.
Am J Kidney Dis.
2002;39(Suppl 1):S1–S266.
Who Should Be Suspected?
Laboratory studies are indicated once renal disease is suspected. Until renal insufficiency is severe, adaptation of tubular function allows excretion of relatively normal amounts of water and sodium.
12-2
).