The Rise and Fall of Modern Medicine (32 page)
Read The Rise and Fall of Modern Medicine Online
Authors: James Le Fanu

The golden age of drug discovery,1940â75
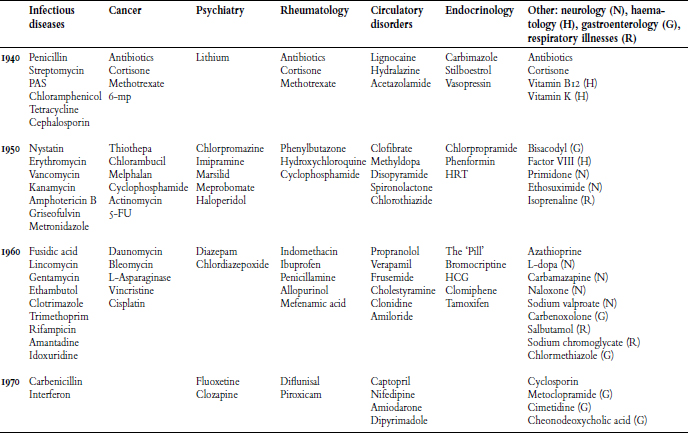
Compounding this frenetic activity was what can best be called the multiplier effect. The more chemicals that were synthesised and the more drugs that were produced, so the greater the chance for the âaccidental' observation, whether in the laboratory or on the ward, that would draw attention to other useful therapeutic avenues to explore. The consequences can be seen in every new edition of the doctor's therapeutic bible, the
Pharmacopoeia
, as by the 1960s over 100 new drugs were being registered each year. But this process could not go on indefinitely. Sooner or later the chemists must run out of new chemicals to test â and then what would happen?
T
ECHNOLOGY'S
T
RIUMPHS
T
echnology, along with drug discovery, shares the prize for the massive expansion of medicine in the post-war years. They are similar, in that both provided empirical solutions to the problems of disease without the necessity for a profound understanding of its nature or causes. They differ, however, in that the manner of technological innovation is almost the precise opposite of drug discovery for, whereas most drugs were discovered by âaccident', technological solutions are, by definition, highly intentional, specific answers to well-defined problems.
Many medical problems proved highly amenable to technological solutions, which subdivide into three categories: Life-sustaining, Diagnostic and Surgical (see opposite). Several have already been encountered, notably the life-sustaining technologies of the intensive-care unit, and particularly the ventilator machine which, by ensuring adequate oxygenation of tissues, can keep people alive during an acute illness until their physiological functions have recovered. Dialysis and the heart pacemaker extend this principle to keeping alive for many
years those with chronic illnesses, such as kidney failure or potentially lethal abnormalities of heart rhythm.
Next, the new methods of diagnostic technology permitted doctors to scrutinise every nook and cranny of the body. The brain, thanks to the CT and MRI scanners, can now be seen with a haunting clarity, while the foetus that previously grew hidden from view within the womb can, thanks to ultrasound, be observed virtually from the moment of conception.
Finally, the surgical technology of the pump and joint replacements, as already described, created respectively the entirely new specialty of cardiac surgery and transformed the scope of orthopaedics.
Three forms of medical technology
| L IFE-SUSTAINING 1 | |
| Intensive care | Dialysis |
| Ventilator | Pacemakers |
| D IAGNOSTIC 2 | |
| CT scanner | PET scanner |
| MRI scanner | Angiography |
| Ultrasound | Cardiac catheterisation |
| S URGICAL 3 | |
| Joint replacement | The pump |
| Intraocular lens implant | Operating microscope |
| Cochlear implant | Endoscopy |
The significance of these technological innovations needs no elaboration. But the most important of all, in the comprehensiveness of its effects, was optics. The Zeiss operating microscope and the endoscope would permit surgeons not only to âsee more' but also to âdo more', and in the process would have a major impact across the whole range of surgical disciplines:
ENT surgery, ophthalmology, neurosurgery, plastic surgery, replantation surgery, gynaecology, orthopaedics and abdominal surgery.
The possibilities of the operating microscope are best conceived by thinking of a household pin whose head is slightly less than 1 mm or 1/20 inch in diameter. Then imagine the pinhead is an artery that has to be sewn on to another artery of the same dimensions. It can't be done. But if the same pinhead-sized arteries are viewed through an operating microscope and magnified twenty-fold then, to the surgeon's eye, both ends now appear to be an inch in diameter, and with delicate instruments they can be sewn together. Welcome to the world of microsurgery.
4
Microsurgery effectively started in 1954, when the German optics company Zeiss produced the first binocular surgical microscope. Among the first to see its possibilities were the ear, nose and throat (ENT) surgeons, for reasons that are readily apparent when leaning over the surgeon's shoulder to watch an operation on a patient with deafness due to hardening of the bones of the middle ear. Peering down the ear canal, the eardrum is readily identifiable as a curtain of tissue. The surgeon takes a knife and cuts away its lower half and then lifts it upwards like a tent flap to expose beneath the three small bones of the middle ear, the most distant of which, the stapes (so called because of its physical resemblance to a rider's stirrups), is in close proximity to the organ of hearing, the semi-circular canals of the inner ear. In otosclerosis, as this patient's condition is called, the stapes becomes immobile and is unable to transmit
the vibrations of sound from the eardrum. The surgeon duly mobilises the stapes by drilling a minute hole through its centre and dropping through a piston whose movements can now transmit the vibrations. It requires little imagination to appreciate how this and similar delicate operations, performed deep within the ear, can only be reliably accomplished with an operating microscope.
5
Next came the ophthalmologists with their immensely successful intraocular lens implant for cataracts which, along with Charnley's hip replacement, became one of the great âmass' operations, tens of thousands being performed every year. In 1948 Harold Ridley, ophthalmic surgeon at St Thomas's Hospital, had a flash of inspiration when a student remarked, after observing him remove a cataract: âIt is a pity the lens cannot be replaced by an artificial one.' Ridley was stimulated by this apparently naive remark to recall his experience from a few years earlier when treating eye injuries in fighter pilots during the Second World War. To his surprise, the fragments of glass from the aircraft's shattered windscreens that had pierced the eyes had caused little damage. Perhaps, Ridley speculated, the eye was some sort of âprivileged sanctuary' that could tolerate foreign objects such as splinters of glass. If so, it would indeed be possible to replace the lens clouded by cataract with a plastic one. His review of his first twenty cases two years later was modestly optimistic, though he did note that âin some the persistence of exudate on the lens surface still partially obstructed vision, but it is not beyond hope that all will become clear in due course'. His medical colleagues took a different view, as his former house surgeon observed: âIt needed great fortitude to face up to the loud criticisms of his colleagues and the frank disbelief at his results.'
6
Ridley's very high failure rate discouraged others, but the
advent of the Zeiss operating microscope in the 1950s and a newer, lighter implant improved results dramatically. âWithout the Zeiss microscope, ophthalmic surgery as it now is would be unimaginable', â not just cataracts, but operations for the relief of glaucoma, for detachment of the retina and on âthe vitreous', the jelly-like substance that maintains the shape of the eyeball.
7
The operating microscope would also prove indispensable for operations involving very small blood vessels, as already described, massively extending the range of three further specialties: neurosurgery, plastic surgery and the replantation of amputated limbs. The first successful replantation operation was performed in Boston in 1962 on a twelve-year-old boy, run over by a train which completely amputated his arm. Eight years later he was arrested by the police âafter using his replanted hand to steal from a store'. The Chinese became particularly adept at this type of surgery, with a report from Shanghai's Sixth People's Hospital of the first hand replantation in 1963 on a 27-year-old man who subsequently went on to become a table-tennis champion.
8
In neurosurgery, the repair of bleeding blood vessels and aneurysms in the brain had always carried a very high mortality rate, but there was not a single fatality in the first forty repairs done with the aid of the operating microscope. âThe importance of the introduction of magnification has completely changed virtually all procedures done within the specialty'.
9
Finally, in plastic surgery, microsurgery revolutionised skin grafting for severe burns, replacing the standard technique devised by Sir Harold Gillies in 1917, when confronted with the problem of reconstructing the face of a sailor severely burned in the Battle of Jutland. âThis poor sailor was rendered hideously repulsive and well nigh incapacitated by his terrible burns. The structure of the nose, lips, eyelids, the ears and neck were burnt
and his hands were contracted into frightful deformity. How a man can survive such an appalling burn is difficult to imagine until one has met one of the survivors from such a fire and realised the unquenchable optimism which carries them through almost anything.' Gillies dissected a skin graft out from a donor site on the sailor's chest except for one end â âthe pedicle' â and then rolled it into a tube, swung it in the direction of the burns on the face and reattached it. The graft's blood supply was maintained by the pedicle until the replanted end had acquired its own blood supply, at which point the graft could then be separated from the pedicle, the tube unrolled and used to cover the mouth and nose.
Gillies was the âfather of plastic surgery' and he trained the following generation just in time for the next major conflict to produce horrifying burns â the Battle of Britain, in 1940. British pilots tumbled out of the air over Kent and into beds at East Grinstead Hospital under the care of one of Gillies's pupils, Sir Archie McIndoe. There they became one of McIndoe's âguinea pigs', so called out of respect for the surgeon under whose care they sometimes remained for two years. Twenty or more separate operations were sometimes necessary, in which pedicles were swung from the arm and shoulder and chest upwards to the face to repair its ravaged appearance. The result was never perfect, though with the passage of time it became more acceptable.
10
Then, quite suddenly, in 1972, these techniques became redundant with the first report of a microsurgical âfree skin flap transfer'. Instead of raising a âtube pedicle' and waiting for it to acquire a new blood supply, the full thickness graft was taken from a part of the body that could afford to lose it â which in the first reported case was the groin â and transferred to the site requiring grafting, the ankle. The minuscule blood vessels of the
graft were then connected â with the aid of the operating microscope â to those of the donor site, the arterial clamps were removed and âthere was immediate perfusion of the graft as evidenced by its colour. After 17 days the sutures were removed and a few luxuriant pubic hairs were noted growing on the ankle. The donor site had completely healed.'
11
The significance of this development scarcely needs to be spelled out as two years of surgery involving up to twenty operations were telescoped down into one procedure.
In summary, the Zeiss operating microscope transformed the practice of ENT, ophthalmology, neurosurgery and plastic surgery. Simultaneously the endoscope, by allowing the visualisation of the internal structures of the body, was having a similar effect on an entirely different range of specialties, including gynaecology, orthopaedics and abdominal surgery.
There are many ways of âseeing' beneath the skin to find out what is amiss in the inner recesses of the body, from the simple chest X-ray to the total-body CT scan, but if the intention is not just to see but also to
do
something, such as cauterising a blood vessel bleeding into the stomach, then there is no alternative other than to use an instrument through which the site of the bleeding can be seen with the human eye and down which a cauterising device can be passed. These instruments are known as âendoscopes', derived from the Greek prefix
endo
â âwithin' â and the verb
skopein
â âto observe' â not merely in the sense of âlooking at something' but also to âobserve with intent'.
There are two types of endoscope, each with its own optical requirements. When the intention is to âobserve with intent' a
hollow organ such as the stomach, colon or bladder, the endoscope must be fully flexible, able to look in all directions and contain an aperture down which a biopsy forceps or a cauterising device can be passed. When, however, the intention is to inspect a closed cavity such as the abdomen to perform some procedure on the female reproductive organs or the gut, then a rigid endoscope is required down which instruments can be passed and whose optics must be of such high quality that it is possible to see what is being operated on with great clarity.