Pediatric Examination and Board Review (213 page)
Read Pediatric Examination and Board Review Online
Authors: Robert Daum,Jason Canel

4.
(A)
Dysuria is frequent, perhaps the most frequent, clinical symptom. Uncircumcised boys are at increased risk compared with circumcised boys, but all boys are at substantially less risk than females in this age group. Fever is usually absent or low grade. High fever accompanied by symptoms and signs of UTI implies pyelonephritis.
5.
(D)
Asymptomatic bacteriuria occurs in about 1% of healthy school girls. The link between it and endstage pyelonephritis has never been convincingly established. Most experts do not believe antimicrobials should be routinely prescribed when asymptomatic bacteriuria is discovered. Careful questioning should be performed, however, to ensure that the patient is truly asymptomatic. Asymptomatic bacteriuria is often cleared spontaneously.
6.
(C)
The traditional definition of pyuria has been more than 5 white blood cells/high power field on centrifuged urine, although modifications have been suggested that can improve the sensitivity and specificity of the test. However, for all ages and for all methods, most children with symptomatic UTI have pyuria. Pyuria is also frequent in patients with Kawasaki disease, measles, and after exercise, however.
7.
(C)
The nitrite dipstick test is highly specific (approximately 98%) for UTI although not reliably sensitive (approximately 50%). It depends on bacteria (gram negatives such as
E coli
,
Klebsiella pneumoniae
, and
Proteus
spp.) converting dietary nitrates to nitrites in the urine specimen and requires a more than 4-hour incubation in the bladder for the reaction to occur. Young children with small bladders frequently void more often. Grampositive bacteria like enterococci do not perform the chemical reaction, and thus the test will not be positive when a gram-positive species is the cause. Urine pH also may be useful in diagnosing UTIs. Urease-producing organisms (eg,
Proteus mirabilis
, some strains of
Staphylococcus saprophyticus
) degrade urea into ammonia, resulting in a high urine pH (8.0-8.5).
8.
(B)
LE has about 80% sensitivity depending on the clinical setting. The specificity is lower, however, because pyuria may yield a positive test (see answer 6). The test is performed only on urine and has no value in the detection of mercury.
9.
(D)
There is no reason to believe that anyone else in the house is at risk from the patient’s
E coli
UTI. Amoxicillin is a poor choice because about half of
E coli
isolates may be resistant. Single-dose therapy of UTI in children has been largely abandoned despite a flurry of onetime interest because the rate of recurrence is unacceptably high. Radiologic studies should be performed in children with a first well-proven UTI. In general, most practitioners perform US and VCUG in a boy of any age with a first UTI, girls younger then 3 with a first UTI, children of any age and gender with a febrile UTI, recurrent UTI, or a UTI with either symptoms referable to the kidney (poor growth, hypertension, abnormal voiding) or a family history of renal disease. A child who has a UTI with fever has a 30-50% likelihood of having underlying vesicoureteral reflux (VUR).
10.
(E)
There is no convincing relationship between reflux and renal scarring, but most experts advocate antimicrobial prophylaxis for patients like this. Amoxicillin is a poor choice for prophylaxis (except in neonates where its side-effect profile is preferred) because enteric organisms have unacceptably high rates of resistance and thus failures are too common. Nitrofurantoin, sulfisoxazole, and trimethoprim-sulfamethoxazole are acceptable choices; no choice will prevent all breakthroughs. Most children with mild to moderate VUR (grades I to III; see
Figure 121-1
) do spontaneously remit (approximately 80% within 5 years), and thus are not usually initially managed with either subureteric transurethral injection (STING procedure) or open surgical reimplantation. Results with the noninvasive, ambulatory STING procedure are good, although they drop off at higher levels of reflux (
Table 121-1
), which are the grades of reflux most often requiring surgical intervention. In the STING procedure, a copolymer substance is injected beneath the mucosa of the ureterovesical junction through a cystoscope.
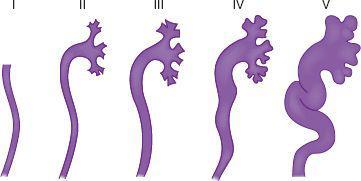
FIGURE 121-1
.
Vesicoureteral reflux. Drawings illustrate the five grades (I-V) of vesicoureteral reflux.
| GRADE VUR | SUCCESS RATE WITH STING PROCEDURE |
| 1, 2 | 79% |
| 3 | 72% |
| 4 | 63% |
| 5 | 51% |
Abbreviations: STING, subureteric transurethral injection; VUR, vesicoureteral reflux.
11.
(A)
Despite the widely held views that all of the choices increase the incidence of UTI, evidencebased data exist to support the relationship between constipation and increased UTI incidence only. Although the other items are frequently advocated by pediatricians, convincing data to support their etiologic relationship are lacking.
12.
(B)
Either by mechanical irritation or by other less well understood mechanisms, pinworms, insertion of foreign bodies into the urethra, and cyclophosphamide can all cause cystitis with symptoms of urgency, frequency, and dysuria. Ibuprofen is the exception. Although a wide variety of toxicities are associated with ibuprofen, cystitis has not been described.
13.
(E)
Although some experts point to the modest in vitro activity of cefazolin against gram negatives, most experts do not rely on this activity for effective therapy for serious infections such as pyelonephritis that are frequently caused by gram negatives.
Pseudomonas
is an unusual cause of UTI and generally not included as an initial target of pyelonephritis therapy. Thus there is no need for ceftazidime. In children, most practitioners would admit and use parenteral antibiotics (often a thirdgeneration cephalosporin). Again, local bacterial susceptibilities should guide empirical selections.
14.
(D)
In theory, no bacteria should be recoverable from urine from a bladder catheterization obtained by sterile technique or from a bladder aspiration. Some clinical microbiology laboratories have introduced a margin of error and use a cutoff of less than 10,000 bacteria per milliliter as a negative culture on bladder urine. Traditionally, more than 100,000 bacteria per milliliter is used as a predictor of bladder infection, although this value was derived from studies done among healthy, asymptomatic adult women. Some have argued that in a symptomatic person (ie, one with dysuria for example), a lower bacterial density (eg, 10,000-100,000) may reflect bladder colonization. Mixed bacterial cultures generally reflect urethral contamination and not any specific disease process, whereas renal and perinephric abscess can be insidious but often present similar to acute pyelonephritis with fever, flank pain, abdominal pain, dysuria, and/or frequency and may be resistant to typical attempts at treatment. See answer 2 for more detail.
15.
(D)
Sexual intercourse and use of a diaphragm with spermicide both increase the risk of UTIs among sexually active females. Neither ingestion of any particular food nor infectious mononucleosis have any demonstrated association with UTIs.
 S
S
UGGESTED
R
EADING
Elder JS, Diaz M, et al. Endoscopic therapy for vesicoureteral reflux: a meta-analysis. I. Reflux resolution and urinary tract infection.
J Urol.
2006;175:716-722.
Gorelick MH, Shaw KN. Screening tests for urinary tract infection in children: a meta-analysis.
Pediatrics.
1999;104:E54.
Hoberman A, Charron M, Hickey RW, et al. Imaging studies after a first febrile urinary tract infection in your children.
N Engl J Med.
2003;348:195-202.
Practice parameter. The diagnosis, treatment, and evaluation of the initial urinary tract infection in febrile infants and young children. American Academy of Pediatrics. Committee on Quality Improvement. Subcommittee on Urinary Tract Infection. [published corrections appear in
Pediatrics
105:141, 2000, 103:1052, 1999, and 104:118, 1999].
Pediatrics.
1999;103(Pt 4 1):843-852.
Report of the International Reflux Study Committee. Medical versus surgical treatment of primary vesicoureteral reflux.
Pediatrics
. 1981;67:392-400.
CASE 122: A 4-MONTH-OLD BOY WITH POOR WEIGHT GAIN, IRRITABILITY, AND LOW URINE OSMOLALITY
A 4-month-old male infant presents with a history of poor weight gain and irritability. He was born at term by vaginal delivery with a birthweight of 3.5 kg. He was breast-fed for 3 months and appeared to have satisfactory weight gain initially. He was then switched to formula feeds, which he has been taking well. Mom says his diapers are always soaking wet. His development has been normal and his immunizations are up to date.
On examination you find an infant who is thin with weight below the 5th percentile and height on the 25th percentile. He appears to be irritable. He has a mildly sunken anterior fontanel, an umbilical hernia, and mild bilateral tibial curvature.
Laboratory studies show the following:
| Hemoglobin | 10.8 g/dL |
| Hematocrit | 32.9% |
| Blood urea nitrogen (BUN) | 17 mg/dL |
| Serum creatinine | 0.5 mg/dL |
| Serum sodium | 148 mEq/L |
| Serum potassium | 3.7 mEq/L |
| Serum chloride | 114 mEq/dL |
| Serum bicarbonate | 20 mEq/dL |
| Serum calcium | 9.8 mg/dL |
| Serum phosphorus | 5.5 mg/dL |
| Serum alkaline phosphatase | 360 U/L |
| Serum magnesium | 1.9 mg/dL |
| Serum glucose | 72 mg/dL |
| Urine specific gravity | 1005 |
| Urine pH | 6.8 |
| Urine osmolality | 198 mOsm/kg of H 2 O |