Pediatric Examination and Board Review (113 page)
Read Pediatric Examination and Board Review Online
Authors: Robert Daum,Jason Canel

(B) use of diphenhydramine the previous day
(C) absence of positive skin controls
(D) history of Stevens-Johnson after penicillin exposure
(E) history of moderate allergic reaction
7.
Which of the following is true regarding RAST testing?
(A) it provides immediate results
(B) the presence of a rash limits its use
(C) it is not affected by steroid use
(D) it has a mild risk of allergic reaction
(E) it can be used with a broad selection of antigens
8.
Besides drug exposure, all of the following are well-known causes of urticarial reaction except
(A) artificial flavoring/coloring
(B) vancomycin
(C) latex
(D) radiocontrast media
(E) all of the above can cause urticaria; no exception
9.
If the boy mentioned in the vignette was having bronchospasm, hypotension, and airway edema, what is the initial treatment of choice?
(A) epinephrine IV (1:1000 dilution)
(B) epinephrine subcutaneous (SC) (1:1000 dilution)
(C) epinephrine IV (1:10000 dilution)
(D) diphenhydramine IV
(E) hydrocortisone IV
10.
Which of the following is not a known etiology of anaphylaxis?
(A) milk ingestion
(B) radiographic contrast media
(C) hymenoptera stings
(D) siphonaptera bites
(E) exercise
11.
All of the following are true regarding the risk for anaphylaxis except
(A) reactions to food occur more frequently among children than adults
(B) atopic children have a higher risk of reactions to drugs than the general population
(C) asthmatic children have a higher risk of reaction to food than the general population
(D) males have a higher risk of reaction to hymenoptera stings than females
(E) a recent exposure to the offending allergen increases the risk of reaction
12.
Which of the following does not support the diagnosis of anaphylaxis?
(A) laryngeal edema, bronchospasm, hypotension
(B) elevated plasma histamine levels
(C) demonstration of immediate hypersensitivity by skin test/RAST
(D) lowered plasma tryptase levels
(E) all of the above are supportive
13.
What is the risk of recurrent anaphylaxis after an episode of anaphylaxis associated with an insect sting?
(A) 20%
(B) 40%
(C) 60%
(D) 80%
(E) 100%
14.
True or False: Large local reactions to insect stings are IgE mediated (allergic)
(A) True
(B) False
15.
Which of the following is true regarding venom skin testing?
(A) it is available only in honeybee and yellow jacket preparations
(B) it indicates reactivity of the patient
(C) testing should be delayed for at least 2 weeks after a reaction from the sting
(D) antihistamines can interfere with results
(E) a negative test excludes the presence of venomspecific IgE antibodies
16.
Which of the following is true regarding radiocontrast media reaction?
(A) the etiology is unknown but appears to be IgEmediated
(B) allergic and asthmatic patients have an increased incidence
(C) reactions are immediate in all cases
(D) anaphylaxis is the most common reaction
(E) approximately 80% experience vasomotor reactions
ANSWERS
1.
(B)
This clinical description is most consistent with accelerated hypersensitivity in the form of urticaria. The proposed mechanism of such a reaction is a delayed type 1 hypersensitivity reaction. Although antibiotics can also cause a type 4 hypersensitivity reaction, the reaction would appear more as a morbilliform, erythematous, pruritic rash with possible associated fever.
2.
(A)
The primary therapy is to discontinue the offending agent. The remaining therapies can all be helpful depending on the extent and severity of the reaction.
3.
(A)
True
4.
(B)
Skin testing is said to be a reliable method for documenting a true penicillin allergy but in practice is seldom performed. Benzylpenicilloyl poly-llysine, the major determinant, is formed as a result of the beta-lactam ring opening. This major determinant is generally responsible for the urticarial reactions, whereas the minor determinants predict anaphylaxis more consistently but are not currently available commercially. Penicillin is the only antibiotic for which skin testing is available.
5.
(C)
Patients who are to undergo skin testing must have ceased taking short-acting antihistamines such as diphenhydramine for at least 48 hours before testing. Generally, medium-acting antihistamines should be stopped for 5 days, and longer-acting antihistamines for 6 weeks. Skin testing may also be clinically affected by long-term corticosteroids, topical steroids, and tricyclic antidepressants.
6.
(E)
Although skin testing is contraindicated in those with severe allergic reaction, a moderate reaction does not limit the use. Those with severe reactions should either be given an alternative drug choice, or if none is available, desensitization without skin testing should be considered.
7.
(C)
RAST is an in vitro option for people who cannot discontinue use of antihistamines or other medications or have conditions such as a rash that interfere with skin testing. It is also useful in those for whom anaphylaxis is a distinct risk. Its disadvantages include the delay in results and the limited specificity to clinically significant antigens.
8.
(E)
All of the substances listed can cause urticaria. Although rapid vancomycin infusion is known to cause red man syndrome (a histamine release syndrome associated with rash and occasionally hypotension), it can have accompanying urticaria.
Latex is being seen more frequently as a cause of allergic reaction, including urticaria and anaphylaxis (see
Figure 69-1
).
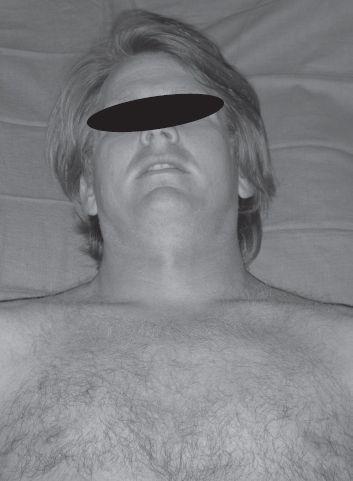
FIGURE 69-1.
Red Man Syndrome. Facial and neck flushing are manifestations that may be seen with red man syndrome from intravenous vancomycin infusion. (Reproduced, with permission, from Knoop KJ, Stack LB, Storrow AS, et al. Atlas of Emergency Medicine, 3rd ed. New York: McGraw-Hill; 2010:576. Photo contributor: R. Jason Thurman, MD.)
9.
(C)
The treatment of choice for severe anaphylaxis, as demonstrated by the symptoms above, is IV epinephrine in 1:10000 dilution, administered every 5-10 minutes while on a cardiac monitor. Initially IM administration of a 1:1000 dilution may be a more available option and should be used when an IV is not yet in place. Hydrocortisone and diphenhydramine are both adjunctive therapies.
10.
(D)
Siphonaptera, or flea bites, are not a known cause of anaphylaxis, although they can cause a significant local reaction. All the remaining items have been known to cause anaphylaxis, including exercise-induced anaphylaxis.
11.
(B)
Although atopic children do have a greater severity of reaction to drugs, they do not have an increased risk of reaction compared with the general public. Males have a higher risk of reaction to stings most likely as a function of their greater exposure to outdoor activities.
12.
(D)
Plasma tryptase levels are elevated in anaphylaxis because tryptase is a protease specific to mast cells. Similarly, histamine is released during mast cell activation.
13.
(C)
14.
(B)
False. Large local reactions to insect stings are not IgE mediated and therefore not allergic in origin. However, once sensitized, a repeat sting may cause symptoms that can progress to IgE release and systemic symptoms.
15.
(D)
Venom skin testing is available in 5 preparations, including honeybee, yellow jacket, yellow hornet, white-faced hornet, and wasp. The testing can only determine prior exposure, not reactivity. A positive test with a strong clinical history is predictive, although a negative test does not exclude the possibility in such a patient. Testing should be delayed for 6 weeks after a reaction. Antihistamines interfere with penicillin skin testing.
16.
(B)
Despite the noted increased incidence of radiocontrast media reactions in allergic and asthmatic patients, recent studies have demonstrated a probably non–IgE-mediated-mechanism. Instead, these reactions are perceived to be mast-cell-mediated. Nonetheless, approximately 5-8% of patients experience some type of immediate vasomotor response, with a small portion having delayed reactions. Urticaria is the most common reaction.
 S
S
UGGESTED
R
EADING