Pediatric Examination and Board Review (112 page)
Read Pediatric Examination and Board Review Online
Authors: Robert Daum,Jason Canel

5.
(E)
All of the foods should be avoided by any breastfeeding mom with a strong family history of food-associated atopic dermatitis, urticaria, or GI disease. Although such avoidances will decrease the incidence of such illness at 1 year, there is no such decrease at 2 years of age.
6.
(C)
Based on the history of night symptoms greater than once a week and possible daily symptoms, this patient would be considered to have moderate persistent asthma. For more information on classification and treatment of asthma, see
http://www.nhlbi.nih.gov/guidelines/asthma
.
7.
(E)
The patient has all the symptoms of an asthma exacerbation with a chest radiograph that is consistent with atelectasis. This requires no additional treatment beyond the treatment for the asthma exacerbation. The use of antibiotics in asthma is reserved for the occurrence of comorbid infections such as sinusitis or bacterial pneumonia.
8.
(E)
Current asthma guidelines recommend a controller medication consisting of an inhaled steroid with a rescue medicine of an inhaled bronchodilator for moderate-persistent asthma. Although leukotriene inhibitors with steroids are recommended as an alternative therapy for moderate-persistent asthma, bronchodilators with inhaled steroid are first-line therapeutic agents.
9.
(B)
It is the opinion of the National Asthma Education and Prevention Program (NAEPP) that asthma education includes the development of an action plan. Key to this plan is the ability to self-assess and manage symptoms and medications. Peak flow measurements and symptom monitoring, individually or in combination, are methods toward this end, and they are recommended for all moderate to severe asthmatics.
10.
(E)
Current studies have demonstrated that low to medium doses of inhaled corticosteroids have no significant adverse effects. Although some studies suggest an association of reduction in linear bone growth with long-term inhaled steroids, this effect is likely nonprogressive and reversible.
11.
(C)
Patients with mild-intermittent asthmatics have symptoms during the day less than 2 times per week with nighttime symptoms twice per week or less, use their albuterol inhaler 2 times per week or less, and have no interference with their regular activity. Pulmonary functions tests (PFTs) show FEV
1
more than 80% of predicted and normal FEV
1
between exacerbations.
12.
(C)
Beta-agonist drugs are part of the treatment plan for asthma. Conversely, beta-adrenergic blocking drugs are known to trigger asthma exacerbations. Weather changes, allergen exposures such as mites, aspirin, and smog can all exacerbate asthma as well.
13.
(B)
There is a 50% chance of atopic disease in a child born to parents who both have an atopic disease. The percentage if one parent has an atopic disease is lower. Those odds increase to 72% if the parents have the same disease. Although 20-30% of the population has an atopic disease, a family history is a strong predictor of a patient’s risk, although environmental influences also play a strong role. Also, when a patient has one atopic disease, he or she has a threefold increase in risk for another atopic disease.
14.
(D)
Both hot and humid and cold and dry climates are risk factors for atopic dermatitis. Atopic dermatitis presents by 2 years of age in about 90% of patients. Allergic rhinitis, the most common atopic disease, is normally preceded by asthma and/or atopic dermatitis, and it is increasing in prevalence in 8- to 13-year-olds.
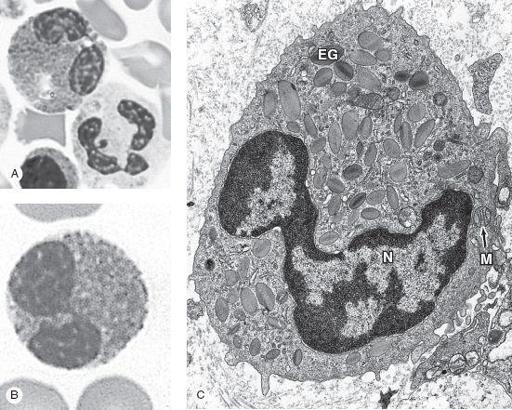
FIGURE 68-1.
Eosinophils. Eosinophils are about the same size as neutrophils but have bilobed nuclei and abundant coarse cytoplasmic granules. The cytoplasm is often filled with brightly eosinophilic specific granules, but also includes some azurophilic granules.
A.
The micrograph shows an eosinophil next to a neutrophil for comparison of its nucleus and granules. X1500. Wright.
B.
Even with granules filling the cytoplasm, the two nuclear lobes of eosinophils are usually clear. X1500. Giemsa.
C.
TEM of a sectioned eosinophil clearly shows the unique specific granules, as oval structures with disk-shaped electron-dense crystalline cores (EG). These along with lysosomes and a few mitochondria (M) fill the cytoplasm around the bilobed nucleus (N). X20,000. (Reproduced, with permission, from Mescher AL. Junquiera’s Basic Histology: Text and Atlas, 12th ed. New York: McGraw-Hill; Fig. 12-9.)
15.
(E)
16.
(E)
Although cidal agents such as benzyl benzoate kill the mites and denature the antigens, the effects are not maintained for prolonged periods, nor are the effects largely significant. These methods are not recommended routinely. The other answer choices are all recommended and proven to be effective in consistently reducing the exposure to dust mites.
17.
(E)
Although all the choices are involved in the pathology of asthma, it is the eosinophil that is the source of major basic protein that injures airway epithelium and enhances bronchial responsiveness (see
Figure 68-1
).
18.
(E)
At least half of all asthmatic children outgrow symptoms by adulthood, although those with severe asthma or multiple allergies are far less likely to do so.
 S
S
UGGESTED
R
EADING
The NAEPP Expert Panel Report Guidelines for the Diagnosis and Management of Asthma—Update on Selected Topics 2007. NIH Publication No. 97-4051. Washington, DC: National Institutes of Health. National Heart Lung and Blood Institute Web site.
http://www.nhlbi.nih.gov/guidelines/asthma/index.htm
. Accessed June 2010.
Lemanske RF Jr, Busse WW. Asthma.
J Allergy Clin Immunol.
2003;111(2 suppl):s502-519.
Nimmagadda SR, Evans RE 3rd. Allergy: etiology and epidemiology.
Pediatr Rev.
1999;20:111-115.
CASE 69: A 5-YEAR-OLD WITH HIVES AFTER 10 DAYS OF ANTIBIOTICS
The mother of a 5-year-old boy calls one summer night to ask about her son’s hives that developed earlier in the evening. The rash is described as red splotches with central clearing. Mom reports that he is itching quite a bit but is breathing well and has no lip involvement. There is no joint pain or abdominal pain. He had a URI 10 days ago and was started on penicillin at a local emergency department yesterday for a “throat infection.” Mom does report that he has been playing outside a lot and has been “getting eaten by bugs.” His diet has not changed significantly, and contains no seafood or peanuts, but he has been drinking a lot of fruit punch. Otherwise he has been doing well with no vomiting, diarrhea, or change in activity or appetite.
SELECT THE ONE BEST ANSWER
1.
Which of the following is the most likely cause of the patient’s rash?
(A) type 1 immediate allergic reaction
(B) type 1 accelerated allergic reaction
(C) type 2 allergic reaction
(D) type 3 allergic reaction
(E) type 4 allergic reaction
2.
The single most important intervention for this patient is
(A) discontinuation of the antibiotic
(B) antihistamines
(C) topical steroids
(D) topical antipruritics
(E) none of the above
3.
True or False. An immediate (<24-hour) reaction to penicillin is most likely IgE-mediated, whereas a reaction occurring later than 24 hours is probably not.
(A) True
(B) False
4.
You decide to test this patient for a penicillin allergy. Which of the following is the most appropriate method for nonemergently diagnosing a penicillin allergy?
(A) penicillin challenge in the intensive care unit (ICU)
(B) skin testing
(C) radioallergosorbent test (RAST)
(D) CAP-RAST testing
(E) none of the above
5.
Regarding skin testing for penicillin allergy, which of the following is false?
(A) negative skin tests occur in most of those with a clinical history
(B) positive skin tests occur in 4% of patients without a clinical history
(C) patients may be tested once off prescription antihistamines for 48 hours
(D) the risk of severe reaction during skin testing is less than 1%
(E) skin testing is more sensitive than RAST testing
6.
Which of the following is not a contraindication to penicillin skin testing?
(A) presence of a diffuse rash