i bc27f85be50b71b1 (88 page)
Read i bc27f85be50b71b1 Online
Authors: Unknown

Table 4-13. Continued
tv
'"
tv
Nerve/Origin
Purpose
How to Test
Signs/Symptoms of lmpairment
>-
Spinal accessory (CN Xl)1
Motor control and proprio
Ask patient to rotate rhe
Weakness with head turn
�
medulla
ception of head rotation,
head or shrug the shouling to the opposite side
r;>
shoulder elevation
ders. Offer gentle resisand ipsilateral shoulder
'"
'"
tance to movement.
shrug
r
,.
Moror control of pharynx
z
"
and larynx
g
Hypoglossal (CN XII)1
Movement and propriocep
Ask the patient ro stick our
fpsilateral deviation of tongue
'"
medulla
tion of tongue for chewhis or her tongue and
during protrusion
o
'"
ing and speech
observe for midline.
Consonant imprecision
Of
Observe for other rongue
;;;
movements.
§
Listen for articulation
r
problems.
Ji
E
eN
'"
= cranjal nerve.
;;i
• R3rd)' tested.
Sources: Data from KW Lindsay, I Bone, R Callander (eds). Neurology and Neurosurgery Illustrated (2nd cd). Edmburgh, UK: Churchill Livingstone, 1991; EN Marieb ted). Human Anatomy and Physiology (5th ed). San Francisco: Benjamin·Cummings, 200 1 ; RJ love, we Webb (eds), Neurology for the Speech-Language Parhologist (4th cd). Boston: Burterworth-Heinemann, 200 I ; and adapted from PA Young, PH
Young (cds). Basic Clinical Neuroanatomy. Baltimore: Williams & Wilkins, 1997;295-297.



NERVOUS SVSfEM
293
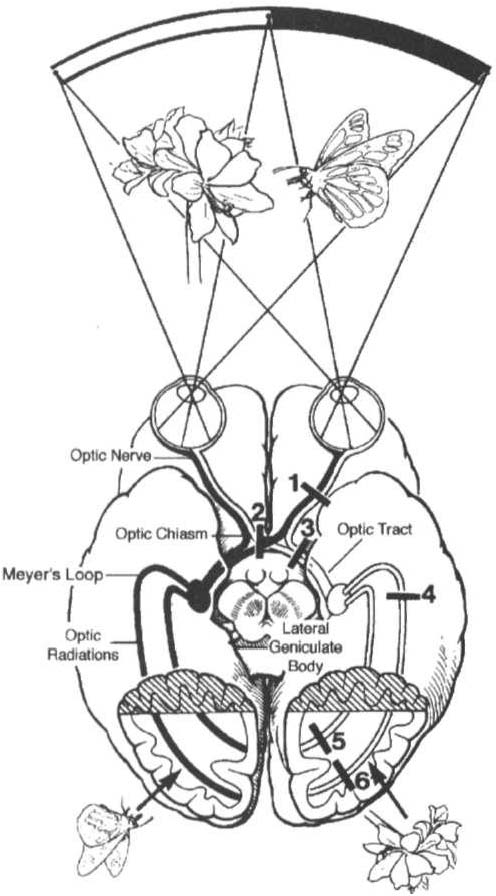
Visual Field Defects
Left Eye Right Eye
1 0
2 () C)
3 () ()
4 � �
5 () ()
6 () ()
Figure 4-7. Visual pathway with lesion sites and resulting visual field defects.
The occipital lobe has been cut away to show the medial aspect aNd the calcarine sulci. (With permission from RJ Love, we Webb leds/. Neurology for the Speech-Language Pathologist 14th ed/. BoStOl1: Butterworth-Heinemann,
2001 ; 1 03.)
of equal size, although up to a 1 -mm difference in diameter can
normally occur between the left and right pupils."
•
Shape. Pupils are normally round but may become oval or irregularly shaped with neurologic dysfunction.
•
Reactivity. Pupils normally constrict in response ro light, as a
consensual response to light shown in the opposite eye or when




294
AClITE CARE HANDBOOK FOR PHYSICAL n IERAPISTS
fixed on a near object. Conversely, pupils normally dilate in the
dark. Constriction and dilation occur briskly under normal cir·
cumstances. A variety of deviations of pupil characteristics can
occur. Pupil reactivity can be tested by shining a light directly into
the patient's eye. Dilated, nonreactive (fixed), malpositioned, or
disconjugate pupils can signify very serious neurologic conditions
(especially oculomotor compression, increased intracranial pressure [ICPJ, or brain herniation) . "
Clinical Tip
•
Note any baseline pupil changes, such as those associated with cataract repair (keyhole shape).
•
If the patient's vision or pupil size or shape changes during physical therapy intervention, discontinue the treatment and notify the nurse or physician immediately.
•
For a patient with diplopia (double vision), a cotton or
gauze eye patch can be worn temporarily over one eye to
improve participation during physical therapy sessions.
•
PERRLA is an acronym that describes pupil function:
pupils equal, round, and reactive to light and accommodation.
Motor Fill/chon
The evaluation of motor function consists of strength, tone, and reflex
testing.
Strength Testing
Strength is the force output of a contracting muscle directly related to
the amount of tension that it can produce. IS Strength can be graded in
the following ways in the acute care setting:
•
Graded 0-5/0-
(normal) with manual muscle testing
•
Graded as strong or weak with resisted isometrics
•
Graded by the portion of a range of motion in which movement
occurs (e.g., hip flexion through one-fourth of available range)
•
Graded functionally