i bc27f85be50b71b1 (279 page)
Read i bc27f85be50b71b1 Online
Authors: Unknown

888 AClJrE CARE HANDBOOK FOR PHYSICAL TIIERAPISTS
world.' The various locations of LE amputation are shown m Figure
V11-1 and are described in Table VlI-l.
Upper-Extremity Amputation
UE amputation is most often the result of trauma, such as automobile or
industrial accidents.' Disease and congenital limb deficiency are also
major causes of UE amputation.2 Despite peripheral vascular disease
being a major cause of LE amputation, it often does nOt create the need
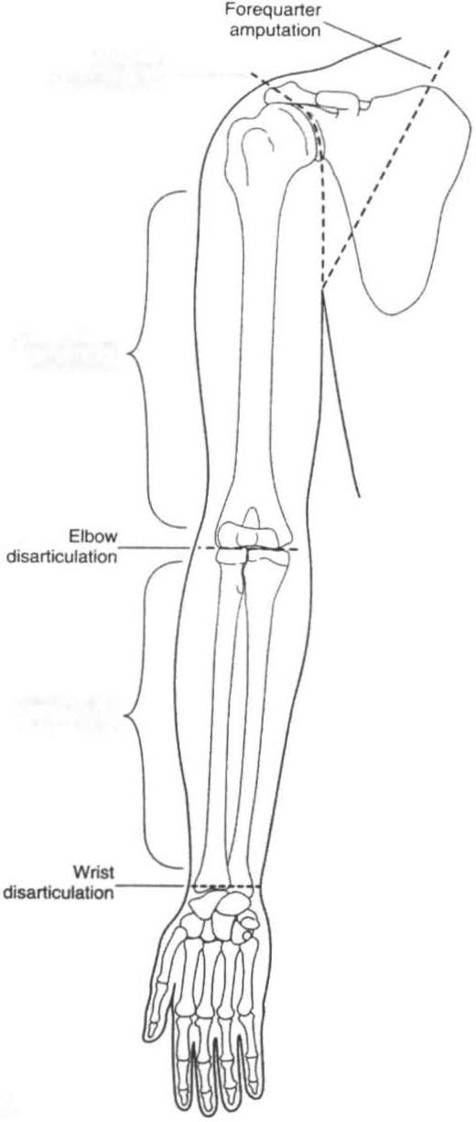
for UE amputation.' The various locations of UE amputations arc shown
in Figure V11-1 and are described in Table vn-2.
Physical Therapy Intervention for Patients
with an Amputation
The focus of physical therapy intervention in the acute care setting is on
preprosthetic evaluation and training. Prosthetic training, if appropriate,
most often occurs in the subacute or horne setting. The primary components of the evaluation for a patient who is status post amputation in the acute care setting are the following':
•
The onset and type of amputation
•
Premorbid lifestyle and functional mobility
•
Currem level of functional mobility
•
Discharge plans
Table V1I-3 outlines general physical therapy considerations and treatment suggestions for the care of patients who experience UE or LE amputations. Table V1I-4 outlines specific clinical concerns for these patients.
APPENDIX VII: AMPlJfATION
889
Shoulder
disartlculatJon'----
Above-elbow
amputation
8ekJw-elbow
amputation
A
Figure VII-t. Levels of amputation, A. Upper extremity. (Reprinted with permission from AB Maher. SW Salmo,Jd, TA Pel/ino /eds), Orthopaedic Nursillg (211d edt. Philadelphia, Sal/llders, 1998;724.)




890 AClITE CARE HANDBOOK FOR PHYSICAL THERAPISTS
Hemipelvectomy
Hip
disarticulation -- -............ _ ..
Above-knee
(translemoral)
amputation
Knee
Below-knee
(transtibial)
amputation
Syme's
Transmetatarsal ____
amputation
Toe
Ray
amputation
B
Figure Vll-l_ Co"tinued. B. LOlller extremity.


APPENDIX VII: AMPlITATION
891
Table VII-I. Types of Lower-Extremity Amputations"
Type
Description
Ray
Single or multiple rays can he amputated depending on
the patient's diagnosis. If the first ray is amputated, halance is often affected, as weight is transferred to the
lateral border of the foot, which may also cause ulceration and skin break down. Postoperative weigln-bearing statuS will range from non-weight bearing to partial weight bearing according to the physician's
orders.
T ransmeratars.11
The metararsal bones are transected with this procedure
as compared to other types of partial foot amputations,
which may disarticulate the metatarsals from the
cuboid and cuneiform bones. Balance is maintained
with a transmetatarsal amputation, because the
residual limb is symmetric in shape and major muscles
remain inract. An adaptive shoe with a rocker-bottom
is used [Q help facilitate push-off in gaiL
S)'me's
Often performed with traumatic and infectious cases, this
amputacion
type of amputation is preferred to more distal, partial
(ankle
foor amputations (Ray and transmetatarsal) because of
disarticulation)
the ease of prosthetic management at this level.
Patients may ambulate with or without a prosthesis.
Below the knee
Ideal site for ampumtion for patienrs with a variery of
(rransribial)
diagnoses. Increased success rate with prosthetic use. In
cases with v3scular compromise, the residual limb may
be slow to heal. Residual limb length ranges from 12.5
cm to 17.5 cm from the knee joinr.
Through-the-knee
Often performed on elderly and young patienrs. M,axi
(disarticulation)
mum prosthetic control can be achieved with this procedure because of the ability [Q fully hear weight on the
residual limb. Also, a long muscular lever arm and
intact hip musculature contribute to great prosthetic
mobility. The intact femoral condyles, however, leave a
cosmetically poor residual limb.
Above the knee
Traditional transfemoral amputation preserves 50--66%
(trans femoral)
of femoral length. Prosthetic amhulation with an
artificial knee joint requires increased metabolic
demand.
Hip
Often performed in cases of trauma or malignancy. The
disarticulation
pelvis remains intact; however, patients may experience
(femoral head
slow wound heeling and may require secondary
from
grafring to fully close the amputation site.
acetabulum)

892 ACUTE CARE HANDBOOK FOR I'HYSICAL THERAPISTS