i bc27f85be50b71b1 (174 page)
Read i bc27f85be50b71b1 Online
Authors: Unknown


GENrrOURINARY SYSTF..M
559
Adrenal
Gland
Ouadratus
Lumborum
Vena
cava
Psoas
Major
Aorta
and
Minor
Figure 9-1. Schematic il/ustration of the genitourinary system, including
trunk musculature. (Artwork by Marybeth Cuaycollg.)
through a process conslstmg of glomerular filtration, tubular reabsorpcion, and tubular sccrecion.1
The following arc the primary functions of the genitourinary system 1,1:
• Excrecion of cellular wasce products (e.g., urea, creacinine [Cr],
and ammonia) through urine formacion and micturition (voiding)
• Regulation of blood volume by conserving or excreting fluids
• Electrolyce regulacion by conserving or cxcrecing minerals


560
ACIJrE CARE HANDBOOK FOR PHYSICAL THFRAPIST�
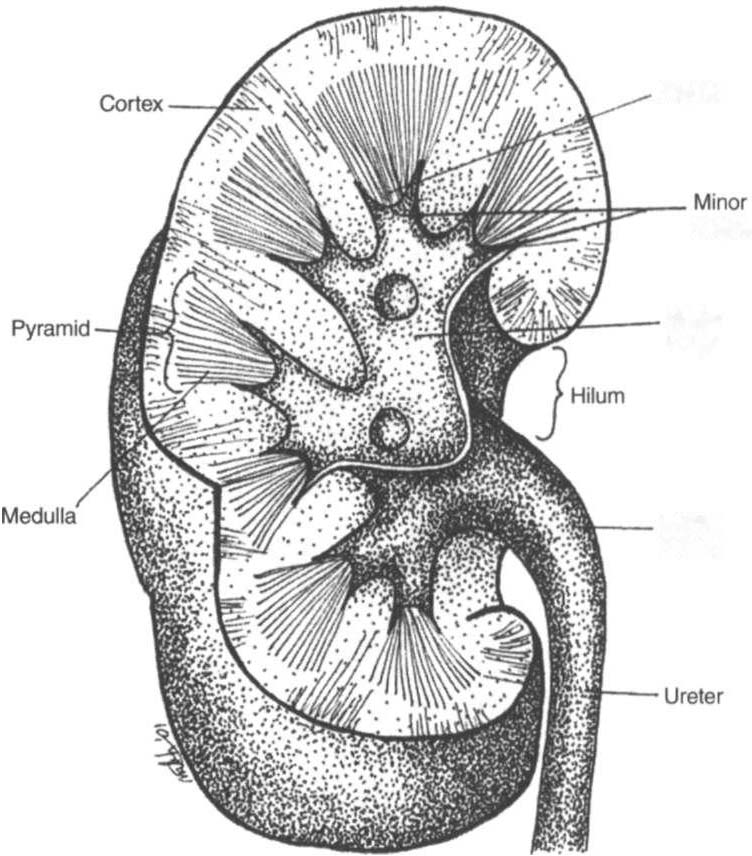
Papilla
calyces
MajOr
Calyx
Renal
Petvis
Figure 9-2. Renal cross section. (Artwork by Marybeth Cuaycong.)
•
Acid-base balance regulation (H' [acidJ and HeOJ Jbase] ions
are reabsorbed or excreted to maintain homeostasis.)
•
Arterial blood pressure regulation (sodium excretion and renin
secretion to maintain homeostasis. Renin is secreted from the kidneys during states of hyporension, which results in formation of angiotensin. Angiotensin causes vasoconstriction to help increase
blood pressure.)
•
Erythropoietin secretion (necessary for stimularing red blood
cell production)
•
Gluconeogenesis (formation of glucose)


GENITOURINARY SYSTEM
561
The brain stem controls micturition through the autonomic nervous
system. Parasympathetic fibers stimulate voiding, whereas sympathetic
fibers inhibit it. The internal urethral sphincter of the bladder and the
external urethral sphincter of the urethra control flow of urine.2
Clinical Evaluation
Evaluation of the genitourinary system involves the integration of
physical findings with laboratory data.
Physical Examillatioll
History
Patients with suspected genitourinary pathology often present with
characteristic complaints or subjective reports. Therefore, a detailed
history, thorough patient interview, review of the patient's medical
record, or a combination of these provides a good beginning to the
diagnostic process for possible genitourinary system pathology. Renal
and urinary pains can vary according to their structural origins; however, they are generally described as pain that is colicky, wave-like, or burning, or occurring as dull aches in the abdomen, back, or buttocks]
Changes in voiding habits or a description of micturition patterns
are also noted and are listed below2-4:
• Decreased force of urinary flow (can indicate obstruction in the
urethra or prostate enlargement)
• Increase in urinary frequency (can indicate obstruction from
prostate enlargement or an acutely inflamed bladder)
• Nocturia (urinary frequency at night, can indicate congestive
heart failure or diabetes mellitus)
• Polyuria (large volume of urine at one time, can indicate diabetes mellitus, chronic renal failure I CRFJ, or excessive fluid intake)
• Oliguria (usually less than 400 ml of urine in a 24-hour period,
can indicate acute renal failure [ARF] or end-stage renal disease
lESRD])
• AliI/ria (less than J 00 ml of urine in a 24-hour period, can indicare severe dehydration, shock, transfusion reaction, kidney disease, or ESRD)




562
AClITE CARE HANDBOOK FOR PHYSICAL THERAPISTS
• Dysuria (pain with voiding, can indicate a wide variety of disorders, including urinary tract infection)
• Hematuria (the presence of blood in urine, can indicare serious
pathology, e.g., cancer or traumatic Foley catheterization. In either
case, the physician should be notified. Refer to Appendix Table