Full House (6 page)

4
Case One: A Personal Story
Where any measure of central tendency acts as a harmful abstraction, and variation stands out as the only meaningful reality
In 1982, at age forty, I was diagnosed with abdominal mesothelioma, a rare and "invariably fatal" form of cancer (to cite all official judgments at the time). I was treated and cured by courageous doctors using an experimental method that can now save some patients who discover the disease in an early stage.
The cancer survivors’ movement has spawned an enormous literature of personal testimony and self-help. I value these books, and learned much from them during my own ordeal. Yet, although I am a writer by trade, and although no experience could possibly be more intense than a long fight against a painful and supposedly incurable disease, I have never felt any urge or need to describe my personal experiences in prose. Instead, as an intensely private person, I view such an enterprise with horror. In all the years then and since, I have been moved to write only one short article about this cardinal portion of my life.
I accept and try to follow the important moral imperative that blessings must be returned with efforts of potential use to others. I am therefore enormously grateful that this article has been of value to people, and that so many readers have requested copies for themselves, or for a friend with cancer. But I did not write my article either from compulsion (as a personal testimony) or from obligation (to the moral requirement cited above). I wrote my piece, The Median Is Not the Message, from a different sort of intellectual need. I believe that the fallacy of reified variation—or failure to consider the "full house" of all cases—plunges us into serious error again and again: my battle against cancer had begun with a fine example of practical benefits to be gained by avoiding such an error, and I could not resist an urge to share the yarn.
We have come a long way from the bad old days, when cancer diagnoses were scrupulously hidden from most patients—both for the lamentable reason that many doctors regarded deception as a preferred pathway for maintaining control, and on the compassionate (if misguided) assumption that most people could not tolerate a word that conveyed ultimate horror and a sentence of death. But we cannot overcome obstacles with ignorance: consider what Franklin D. Roosevelt could have contributed to our understanding of disability if he had not hidden his paralysis with such cunning care, but had announced instead that he did not govern with his legs.
American doctors, particularly in intellectual centers like Boston, now follow what I regard as the best strategy for this most difficult subject: any information, no matter how brutal, will be given upon request (as compassionately and diplomatically as possible, of course); if you don’t want to know, don’t ask. My own doctor made only one departure from this sensible rule—and I forgave her immediately as soon as I faced the context. At our first meeting, after my initial surgery, I asked her what I could read to learn more about mesothelioma (for I had never heard of the disease). She replied that the literature contained nothing worth pursuing. But trying to keep an intellectual from books is about as effective as that old saw about ordering someone not to think about a rhinoceros. As soon as I could walk, I staggered over to the medical school library and punched mesothelioma into the computer search program. Half an hour later, surrounded by the latest articles, I understood why my doctor had erred on the side of limited information.
All the literature contained the same brutal message: mesothelioma is incurable, with a median mortality of eight months following diagnosis. A hot topic of late, expressed most notably in Bernie Siegel’s best-selling books, has emphasized the role of positive attitude in combating such serious diseases as cancer. From the depths of my skeptical and rationalist soul, I ask the Lord to protect me from California touchie-feeliedom. I must, nonetheless, express my concurrence with Siegel’s important theme, though I hasten to express two vital caveats. First, I harbor no mystical notions about the potential value of mental calm and tenacity. We do not know the reasons, but I am confident that explanations will fall within the purview of scientific accessibility (and will probably center on how the biochemistry of thought and emotion feed back upon the immune system). Second, we must stand resolutely against an unintended cruelty of the positive attitude" movement—insidious slippage into a rhetoric of blame for those who cannot overcome their personal despair and call up positivity from some internal depth. We build our personalities laboriously and through many years, and we cannot order fundamental changes just because we might value their utility: no button reading "positive attitude" protrudes from our hearts, and no finger can coerce positivity into immediate action by a single and painless pressing. How dare we blame someone for the long-standing constitution of their tendencies and temperament if, in an uninvited and unwelcome episode of life, another persona might have coped better? If a man dies of cancer in fear and despair, then cry for his pain and celebrate his life. The other man, who fought like hell and laughed to the end, but also died, may have had an easier time in his final months, but took his leave with no more humanity.
My own reaction to reading this chillingly pessimistic literature taught me something that I had suspected, but had not understood for certain about myself (for we cannot really know until circumstances compel an ultimate test): I do have a sanguine temperament and a positive attitude. I confess that I did sit stunned for a few minutes, but my next reaction was a broad smile as understanding dawned: "Oh, so that’s why she told me not to read any of the literature!" (My doctor later apologized, explaining that she had erred on the side of caution because she didn’t yet know me. She said that if she had been able to gauge my reaction better, she would have photocopied all the reprints and brought them to my bedside the next day.)
My initial burst of positivity amounted to little more than an emotional gut reaction—and would have endured for only a short time, had I not been able to bolster the feeling with a genuine reason for optimism based upon better analysis of papers that seemed so brutally pessimistic. (If had read deeply and concluded that I must inevitably die eight months hence, I doubt that any internal state could have conquered grief.) I was able to make such an analysis because my statistical training, and my knowledge of natural history, had taught me to treat variation as a basic reality, and to be wary of averages—which are, after all, abstract measures applicable to no single person, and often largely irrelevant to individual cases. In other words, the theme of this book—"full house," or the need to focus upon variation within entire systems, and not always upon abstract measures of average or central tendency—provided substantial solace in my time of greatest need. Let no one ever say that knowledge and learning are frivolous baubles of academic sterility, and that only feelings can serve us in times of personal stress.
I started to think about the data, and the crucial verdict of "eight months’ median mortality" as soon as my brain started functioning again after the initial shock. And I followed my training as an evolutionary biologist. Just what does "eight months median mortality" signify? Here we encounter the philosophical error and dilemma that motivated this book. Most people view averages as basic reality and variation as a device for calculating a meaningful measure of central tendency. In this Platonic world, "eight months’ median mortality" can only signify: "I will most probably be dead in eight months"—about the most chilling diagnosis anyone could ever read.
But we make a serious mistake if we view a measure of central tendency as the most likely outcome for any single individual—though most of us commit this error all the time. Central tendency is an abstraction, variation the reality. We must first ask what "median" mortality signifies. A median is the third major measure of central tendency. (I discussed the other two in the last chapter—the mean, or average obtained by adding all the values and dividing by the number of cases; and the mode, or most common value.) The median, as etymology proclaims, is the halfway point in a graded array of values. In any population, half the individuals will be below the median, and half above. If, say, in a group of five children, one has a penny, one a dime, one a quarter, one a dollar, and one ten dollars, then the kid with the quarter is the median, since two have more money and two less. (Note that means and medians are not equal in this case. The mean wealth of $2.27—the total cash of $11.36 divided by five—lies between the fourth and fifth kids, for the tycoon with ten bucks overbalances all the paupers.) We favor medians in such cases, when extension at one end of the variation drags the mean so far in that direction. For mortality in mesothelioma and other diseases, we generally favor the median as a measure of central tendency because we want to know the halfway point in a series of similar outcomes graded in time. A higher mean might seem misleading in the case of mesothelioma because one or two people living a long time (the analog of the kid with ten bucks) might drag the mean to the right and convey a false impression that most people with the disease will live for more than eight months—whereas the median correctly informs us that half the afflicted population dies within eight months of diagnosis.
We now come to the crux of practice: I am not a measure of central tendency, either mean or median. I am one single human being with mesothelioma, and I want a best assessment of my own chances—for I have personal decisions to make, and my business cannot be dictated by abstract averages. I need to place myself in the most probable region of the variation based upon particulars of my own case; I must not simply assume that my personal fate will correspond to some measure of central tendency.
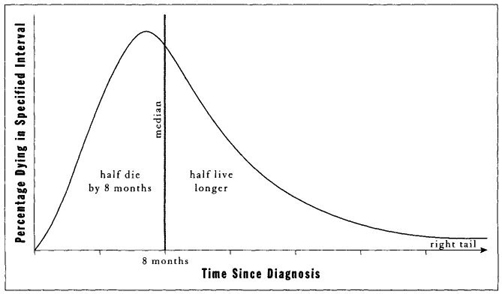
I then had the key insight that proved so life-affirming at such a crucial moment. I started to think about the variation and reasoned that the distribution of deaths must be strongly "right skewed" in statistical parlance—that is, asymmetrically extended around a chosen measure of central tendency, with a much wider spread to the right than to the left. After all, there just isn’t much room between the absolute minimum value of zero (dropping dead at the moment of diagnosis) and the median value of eight months. Half the variation must be scrunched up into this left half of the curve (see Figure 4) between the minimum and the median. But the right half may, in principle, extend out forever, or at least into extreme old age. (Statisticians refer to the ends of such distribution as "tails"—so I am saying that the left tail abuts a wall at zero survivorship, while the right tail has no necessary limit but the maximal human life span.)
I needed, above all, to know the form and expanse of variation, and my most probable position within the spread. I realized that all factors favored a potential location on the right tail — I was young, rarin’ to fight the bastard, located in a city offering the best possible medical treatment, blessed with a supportive family, and lucky that my disease had been discovered relatively early in its course. I was therefore far more interested in the right tail (my probable residence) than in any measure of central ten
-
dency (an abstraction with no special relevance to my case). What, then, could possibly be more uplifting than an inference that the spread of variation would be strongly right skewed? I then checked the data and confirmed my supposition: the variation was markedly right skewed, with a few people living a long time. I saw no reason why I shouldn’t be able to reside among these inhabitants of the right tail.
This insight gave me no guarantee of normal longevity, but at least I had obtained that most precious of all gifts at a crucial moment: the prospect of substantial time—to think, to plan, and to fight. I would not immediately have to follow Isaiah’s injunction to King Hezekiah: "Set thine house in order: for thou shalt die, and not live." I had made a good statistical inference about the importance of variation and the limited utility of averages, and I had been able to confirm this suspicion with actual data. I had used knowledge and gained succor. (This story boasts an even more favorable outcome. I was destined for the right tail anyway, but an experimental treatment worked and has now probably removed the disease entirely. Old distributions offer no predictions for new situations. I trust that I am now headed for the right tail of a new distribution based on this successful treatment: death at a ripe old age in two high figures— maybe even three low ones.)
I present this tale not only for the pleasure of retelling a crucial yarn about my life, but because it encapsulates all the principles that form the core of this book. First of all, my story illustrates the importance of variation within whole systems as an ultimate reality—and the limited utility (and abstract nature) of averages. Moreover, in a didactic sense for this book, my story embodies the three terms and concepts that form the conceptual apparatus for all the examples to follow. Let me try, then, to present these principles in a formal way, and in a context that will not seem too dry or forbidding.