Dead Men Do Tell Tales: The Strange and Fascinating Cases of a Forensic Anthropologist (44 page)
Read Dead Men Do Tell Tales: The Strange and Fascinating Cases of a Forensic Anthropologist Online
Authors: William R. Maples,Michael Browning
Tags: #Medical, #Forensic Medicine

An incomplete gunshot exit wound. Note fractures near top of cranium. The round entrance wound from a second bullet shows no external beveling of the bone surface.
A 12 gauge shotgun entrance wound, fired from about ten feet away from the victim.
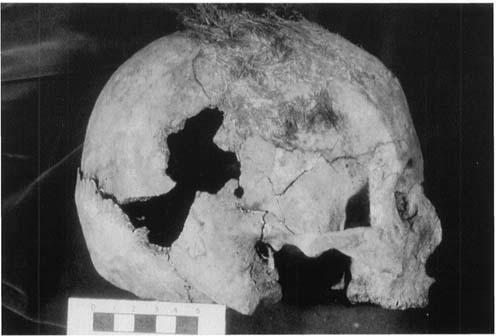
Skull showing multiple fractures from a tool.
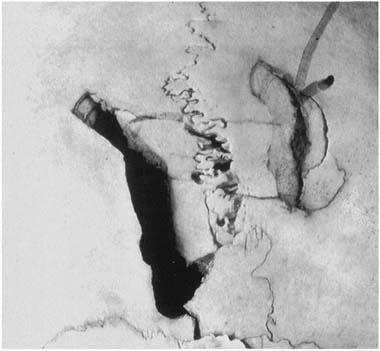
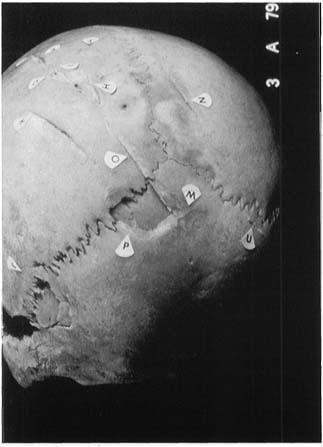
Which injury came first? This closeup photograph shows the injury on the left occurred before that on the right because a fracture (see arrow) from the left injury crosses the injury on the right. Therefore the blow on the left fell first.
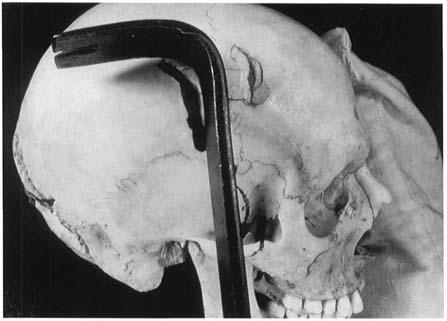
An apparent mismatch. When the tool is placed next to the wounds, it is not consistent. It has a right-angle bend. Such a tool would have cut smoothly into thin bone. Note that the top of the tool is ground down (dressed) while the shaft of the tool remains rounded.
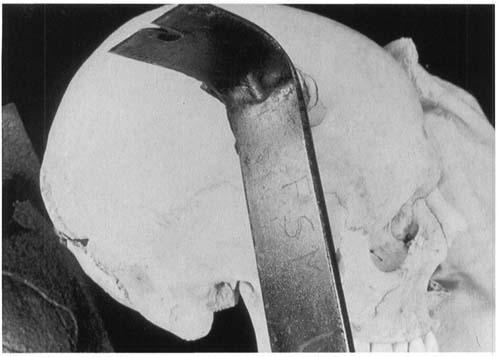
When the tool is rotated, however, the effective angle is now greater than 90 degrees. The tool would now crush the bone, causing the sloping surfaces seen in the wound.

A gunshot exit wound, producing outer beveling of bone surfaces.
Multiple wounds from a meat cleaver.
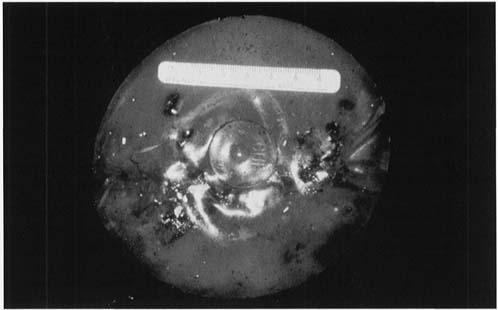
The size and manufacturer’s trademark can be seen near the center of a silicone breast augmentation implant. One of my students once mistook this implant for a jellyfish.

The many large white areas in this radiograph are scattered bullet fragments from multiple rounds of a .22 in the head.
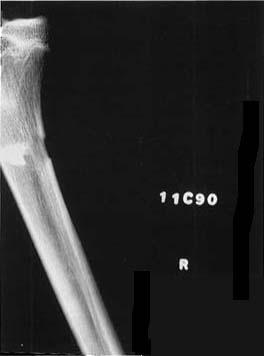
A .22 bullet can be seen embedded in a bone from the leg. The entrance wound in the back of the bone suggests that the victim may have been running from the assailant when he was shot.
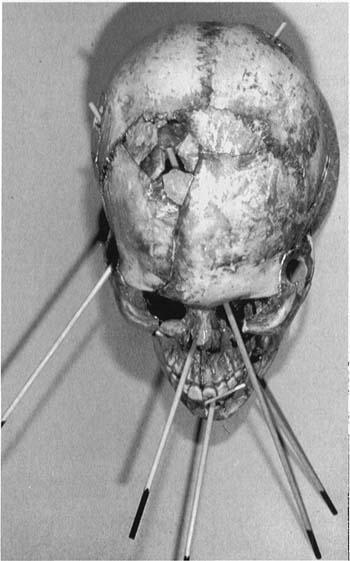
The bullet tracks of five .22-caliber wounds to the head are indicated by the dowel pins.

Vertebrae from the chest of an elderly man showing bony outgrowths on the bodies and fusion of many vertebrae. In life, this man’s movements would have been severely limited.
