Resident Readiness General Surgery (55 page)
Read Resident Readiness General Surgery Online
Authors: Debra Klamen,Brian George,Alden Harken,Debra Darosa
Tags: #Medical, #Surgery, #General, #Test Preparation & Review

4.
The “4-2-1 Rule” is a quick way to estimate volume replacement (see
Figure 42-1
).
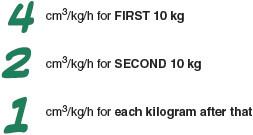
Figure 42-1.
4-2-1 Rule for estimates of maintenance fluid requirements.
Using this rule for Ms. Yang gives us:

In clinical practice the maintenance fluid requirement is then often adjusted based on the estimated quantity of other losses. For example, patients with high NGT outputs often receive 1 cm
3
: 1 cm
3
replacement for their NGT fluid losses in addition to their maintenance fluids. For Ms. Yang, this would mean receiving a 600 cm
3
bolus in addition to her 120 cm
3
/h maintenance fluid rate. The 600 cm
3
loss can also be added incrementally over 24 hours (600 cm
3
/24 hours = 25 cm
3
/h + 120 cm
3
/h = 145 cm
3
/h maintenance fluid rate). It is important to note that the “4-2-1 Rule” provides only an estimate and that estimate should be used for initial maintenance fluid administration, not to calculate resuscitation requirements.
When the formula is used to calculate initial maintenance rates, adequate volume replacement must still be continually reassessed. The goal of adequate volume replacement, as discussed in the chapter on Shock, is to optimize preload and thereby optimize cardiac output and end-organ perfusion. For this reason, urine output (a measure of renal perfusion) is often used to determine when adequate volume replacement has been achieved. It should be maintained at least to 0.5 cm
3
/kg/h.
5.
Certain patient populations require special attention when being resuscitated postoperatively or when calculating maintenance fluid requirements because they have increased risks for volume overload. Patients with poor cardiac function or patients on dialysis are especially susceptible to this complication. Oftentimes in clinical practice these patients receive fluids based on ideal body weight (IBW) that adjusts body weight based on height.
One of the first signs of volume overload is weight gain. The excess fluid can also cause swelling in the extremities manifested as peripheral edema. Excess fluid can also enter the air spaces of the lungs and compromise oxygenation leading to shortness of breath. This can manifest as crackles on physical exam. Finally, when fluid overload is significant, there may be cardiac compromise in the form of arrhythmias such as atrial fibrillation or the development of congestive heart failure.
6.
Diabetic patients are another patient population requiring special caution when IV fluids are being administered. Because this patient population receives exogenous insulin to control blood glucose levels, extra care must be taken to avoid hypoglycemia when patients are NPO. Adding dextrose to the maintenance fluid of diabetic patients ensures they do not “bottom out” their blood glucose
levels. Furthermore, just as with nondiabetic patients, small amounts of dextrose help prevent the diabetic patient who is NPO from going into “starvation mode” and entering a catabolic state.
TIPS TO REMEMBER
Both NS and LR are isotonic crystalloid solutions. LR solution is similar to plasma in electrolyte composition (ie, it includes potassium, bicarbonate, and calcium).
Other books
Crown of Steel (Chaos Awakens) by Heath Pfaff
Life After That by Barbara Kevin
Reason to Breathe by Rebecca Donovan
Munich Airport by Greg Baxter
The Might Have Been by Joe Schuster
All Roads Lead Home by Wasowski, Mary
Hudson by Laurelin Paige
The Harrowing of Gwynedd by Katherine Kurtz
Synthetic: Dark Beginning by Shonna Wright
St. Urbain's Horseman by Mordecai Richler