i bc27f85be50b71b1 (97 page)
Read i bc27f85be50b71b1 Online
Authors: Unknown

320
AClITE CARE HANDBOOK FOR I)HYSICAL THERAPISTS
Guillain-Barre Syndrome
Guillain-Barre syndrome (GBS), or acute inflammatory demyelinating polyradiculopathy, is caused by the breakdown of Schwann cells by antibodies." There is an onset of paresthesia, pain (especially of
the lumbar spine), symmetric weakness (commonly proximal followed by distal, including the facial and respiratory musculature), and autonomic dysfunction approximately 1-3 weeks afrer a viral
infection. GBS is diagnosed by history, clinical presentation, CSF
sampling (increased protein level), and EMG studies (which show
decreased motor and sensory velocities).' Once diagnosed, the
patient with GBS is hospitalized because of the potential for rapid
respirarory muscle paralysis.4S Functional recovery varies from full
independence to residual weakness that takes J 2-24 months to
resolve." GBS is fatal in 5% of cases.'s The management of GBS
may consist of pharmacologic therapy (immunosuppressive agents),
plasma exchange, intravenous immunoglobulin, respiratory support, physical therapy, and the supportive treatmenr of associated symptoms (e.g., pain management).
Multiple Sclerosis
MS is the demyelination of the white maner of the CNS and of the
optic nerve, presumably an autoimmune reaccion. MS is categorized
by onset and progression as relapsing-remitting (clearly defined
relapses with full recovery or with residual deficit), primary progressive (occasional plateaus in disease progression and only temporary improvements), secondary progressive (initial relapsing-remitting followed by disease progression with or without relapses or plateaus), or progressive relapsing (progressive from onset with acute relapses,
with or without full recovery) J4
MS typically occurs in 20- to 40-year-olds and in women more
than men. It is diagnosed by history (the onset of symptoms must
occur and resolve more than once), clinical presentation, CSF sampling (increased myelin protein and immunoglobulin G levels), and by M R I (which shows the presence of two or more plaques of the
CNS).' These plaques are located at areas of demyelination where
lymphocytic and plasma infiltration and gliosis have occurred. Signs
and symptoms of the early stages of MS may include focal weakness, fatigue, diplopia, blurred vision, equilibrium loss (vertigo), and urinary incontinence. Additional signs and symptoms of the larrer
stages of MS may include ataxia, paresthesias, spasticity, sensory
deficits, hyper-reflexia, tremor, and nysragmus.44 The management
NERVOUS SYSTEM
321
of MS may include pharmacologic therapy (corticosteroids), skeletal
muscle relaxants, physical therapy, and the treatment of associated
disease manifestations (e.g., bladder dysfunction).
Parkinson's Disease
Parkinson 's disease (PO) is the idiopathic progressive onset of
bradykinesia, altered posture and postural reflexes, resting tremor,
and cogwheel rigidity. Other signs and symptoms may include shuffling gait characterized by the inability to start or stop, blank facial expression, drooling, decreased speech volume, an inability to perform fine motor tasks, and dementia." PO is diagnosed by history, clinical presentation, and MRI (which shows a light rather than
dark substantia nigra).8 The management of PO mainly includes
pharmacologic therapy with anti parkinsonian agents and physical
therapy. Stereotactic thalamotomy and the placement of a highfrequency thalamic stimulator are surgical options for symptoms refractory to medical therapy."
General Management
11.tracrallial and Cerebral Perfusion Pressure
The maintenance of normal [CP or the prompt recognition of elevated [CP is one of the primary goals of the team caring for the postcraniosurgical patient or the patient with cerebral trauma, neoplasm, or infection.
ICP is the pressure CSF exerts within the ventricles. This pressure
(normally 4- 1 5 mm Hg) fluctuates with any systemic condition, body
position, or activity that increases cerebral blood flow, blood pressure, or intrathoracic or abdominal pressure or that decreases venous return or increases cerebral metabolism.
The three dynamic variables within the fixed skull are blood, CSF,
and brain tissue. As [CP rises, these variables change in an attempt to
lower [CP via the following mechanisms: cerebral vasoconstriction,
compression of venous sinuses, decreased CSF production, or shift of
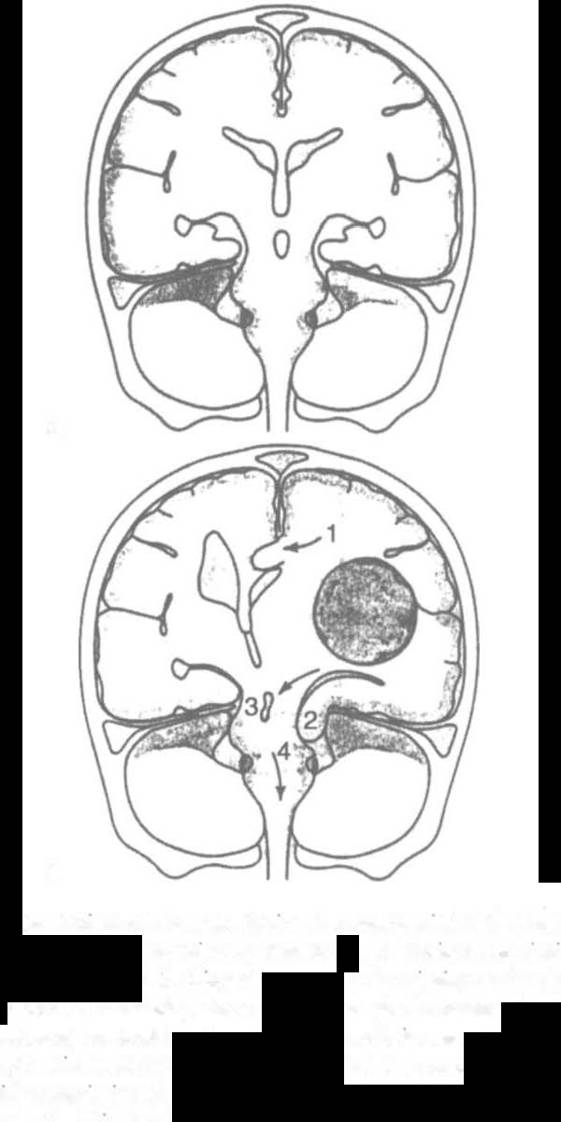
CSF to the subarachnoid space. When these compensations fail, compression of brain structures occurs, and fatal brain herniation will develop if untreated (Figure 4-8). The signs and symptoms of
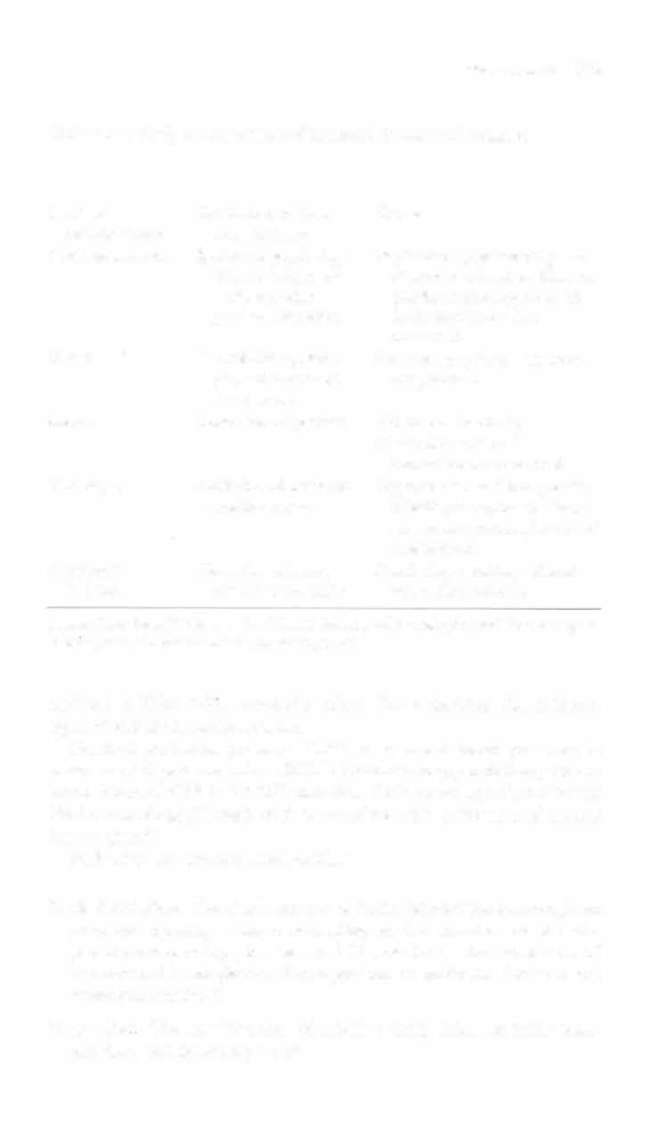
increased [CP are listed in Table 4-20. The methods of controlling
Iep, based on clinical neurologic examination and diagnostic tests, are


322 ACUTE CARF HANDBOOk foOR I'HYSICAI THfoRAI)I\P,
A
B
Figure 4·8. Herniat toll syndromes depIcted. tntracramaJ shIlts from supraten·
toriaJ lesions. A. N ormal locatIo" of structures. B. Vanous hermatloll sy,,·
dromes are demonstrated. I . Cmgulate gyrus is hermatmg under falx cerebrt.
2. Temporal lobe is hermatmg dowtlluard through the te"torial notch.
J. CompressIon of contralateral cerebral peduncle IS seen. 4. Downward d,s·
placement of bram stem through tentorial notch ;s a central herniatIOn syn·
drome. ( W ,th permlsS/on (rom PC Beare, lL M)'ers {eds{. Adllit Health
NI/rsmg {3rd ed{. Pllliodelpl"a , Sal/llders, 1 998;919.}

NERVOUS SYSTEM
323
Table 4-20. Early and Lare Signs of Increased Intracranial Pressure
Observation
Early
Late
Level of
Confusion, restless
Coma
consciousness
ness, lethargy
Pupil appearance
Ipsilateral pupil slug
Papilledema, ipsilateral pupil
gish ro light, ovoid
dilated and fixed or bilateral
in shape. with
pupils dilated and fixed (if
gradual dilatation
brain herniation has
occurred)
Vision
Blurred vision, diplo
Same as early signs but more
pia, and decreased
exaggerated
visual acuity
Moror
Contralateral paresis
Abnormal posturing
Bilateral flaccidity if
herniation has occurred
Vital signs
Stable blood pressure
Hypertension and bradycardia
and hean rate
(Cushing's response), altered
respirarory pattern, increased
temperature
Additional