Wallach's Interpretation of Diagnostic Tests: Pathways to Arriving at a Clinical Diagnosis (387 page)
Authors: Mary A. Williamson Mt(ascp) Phd,L. Michael Snyder Md

Who Should Be Suspected?
Patients with cold-induced thrombotic events or patients with painful ulcers, purpura, livedo reticularis, and painful or pruritic erythema of the extremities. The disease is common in patients with HCV. An individual whose plasma, but not serum, forms a cryoprecipitate has cryofibrinogenemia. Some individuals may be asymptomatic, and CF may be discovered accidentally in the laboratory.
Refer to Cryoglobulins in Chapter
16
.
Suggested Reading
Peng SL. Cryofibrinogenemia. In: Basow DS (ed).
UpToDate
, Waltham, MA: UpToDate, Inc.: 2013.

DISORDERS OF HEMOSTASIS AND THROMBOSIS
DISORDERS OF PLATELETS: THROMBOCYTOPENIAS
Thrombocytopenias represent a reduction in the number of circulating platelets below the lower limit of normal set by the laboratory (see p. 1083). They may be classified in various ways. First one must determine if the condition is congenital or acquired. Acquired thrombocytopenias may be acute or chronic. The causes of thrombocytopenias can be classified by etiology (Figure
9-3
): increased destruction, decreased production, artifactual, and miscellaneous. TTP/HUS is discussed separately (see p. 467).
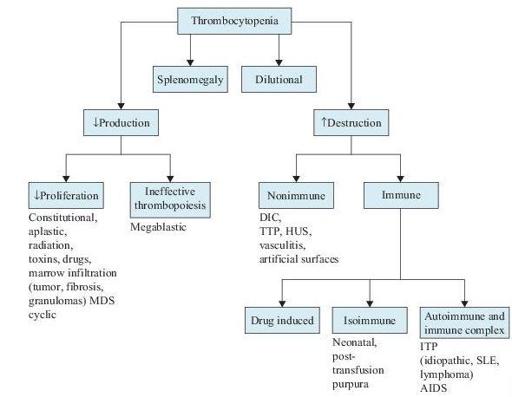
Figure 9–3
The etiology of thrombocytopenia. DIC, disseminated intravascular coagulation; HUS, hemolytic uremic syndrome; TTP, thrombotic thrombocytopenic purpura; MDS, myelodysplastic syndromes.
IMMUNE THROMBOCYTOPENIC PURPURA (ITP)
ITP is an autoimmune disease characterized by a low platelet count (<150 × 10
9
/L) due to their accelerated destruction and impaired platelet production. Typically, thrombocytopenia is isolated without other hematopoietic lineages being affected. Depending on the severity of thrombocytopenia and other contributing factors, patients with ITP are at increased risk for bleeding. There is marked interpatient variability in the clinical presentation of ITP. Although the onset may be abrupt, it is more often insidious. ITP is a heterogeneous group of disorders. Most cases are considered primary, whereas others are secondary to drugs, other autoimmune conditions such as SLE, or HIV, HCV CMV, and VZV infections.
Individuals with no previous history of bleeding and no hematologic disease who complain of mucosal (especially epistaxis, gum, or excessive menstrual bleeding) and subcutaneous bleeding in the form of petechiae or ecchymosis. Splenomegaly or lymphadenopathy is not present.
In children, ITP is often preceded by a viral infection, and most cases remit spontaneously.
Gestational thrombocytopenia occurs in mid-second to third trimester. It is generally mild. Its etiology is unclear. TTP or thrombocytopenia associated with preeclampsia must be ruled out.
Laboratory findings are not specific; there is no “gold standard” test that can reliably establish the diagnosis.
RBC: normal count, unless the bleeding had been excessive or of long duration in which cases anemia may be present and the reticulocyte count elevated.