Wallach's Interpretation of Diagnostic Tests: Pathways to Arriving at a Clinical Diagnosis (342 page)
Authors: Mary A. Williamson Mt(ascp) Phd,L. Michael Snyder Md


Genomic studies
may emerge in the future as the best tools for determining the clinical course of CLL/SLL. Genetic complexity is associated with aggressive disease. Loss or mutation of TP53 (a tumor suppressing gene) places patients in the highest risk prognostic group. Down-regulation of miR-29c and miR-223, and possibly other microRNAs, has been associated with adverse prognosis. MiR-34a indicates resistance to chemotherapy. This is an area that is developing rapidly. The integration of genomic mutations and cytogenetic lesions improves the accuracy of survival prediction in CLL.
Serum immunoglobulins
: Hypogammaglobulinemia develops and progresses as the disease becomes more advanced. A monoclonal protein, usually of the same class as the surface membrane immunoglobulin, is found in 5% of patients.
TABLE 9–3. Differential Immunophenotypic Markers for Four Chronic Lymphoproliferative Diseases
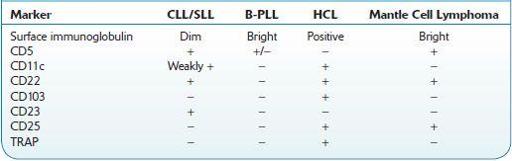
B-PLL, prolymphocytic leukemia; CLL, chronic lymphocytic leukemia; HCL, hairy cell leukemia; SLL, small lymphocytic lymphoma; TRAP, tartrate-resistant acid phosphatase.
Transformation
Suggested Readings
Gribben JG. How I treat chronic lymphocytic leukemia.
Blood.
2010;115:187–197.
Rawstron AC, Bennett FL, O’Connor SJM, et al. Monoclonal B-cell lymphocytosis and chronic lymphocytic leukemia.
N Engl J Med.
2008;359:575–583.
Rossi D, Rasi S, Spina V, et al. Integrated mutational and cytogenetic analysis identifies new prognostic subgroups in chronic lymphocytic leukemia.
Blood.
2013;121:1403–1412.
Rossi D, Spina V, Deambrogy C, et al. The genetics of Richter syndrome reveals disease heterogeneity and predicts survival after transformation.
Blood.
2011;117:3391–3401.
PROLYMPHOCYTIC (PLL) LEUKEMIA OF B- AND T-CELL SUBTYPE
B-cell PLL is a rare, aggressive, clonal lymphoproliferative disease composed mainly of B-cell prolymphocytes. It involves peripheral blood, bone marrow, and spleen. T-cell PLL is still rarer and will not be discussed further.
Patients who present with prominent splenomegaly but no lymphadenopathy, B symptoms and WBC counts of >100,000 comprised nearly exclusively of abnormal appearing lymphocytes and frequently with anemia and thrombocytopenia. Some have a history of CLL/PLL, which occasionally transforms into B-cell PLL (see p. 402).
CBC
: 50% of patients present with anemia and thrombocytopenia.