Wallach's Interpretation of Diagnostic Tests: Pathways to Arriving at a Clinical Diagnosis (236 page)
Authors: Mary A. Williamson Mt(ascp) Phd,L. Michael Snyder Md

BOOK: Wallach's Interpretation of Diagnostic Tests: Pathways to Arriving at a Clinical Diagnosis
2.92Mb size Format: txt, pdf, ePub
Cystine stones are rare, occurring in patients with homozygous congenital familial cystinuria, and characterized by bilateral obstructive staghorn calculi with associated renal failure.
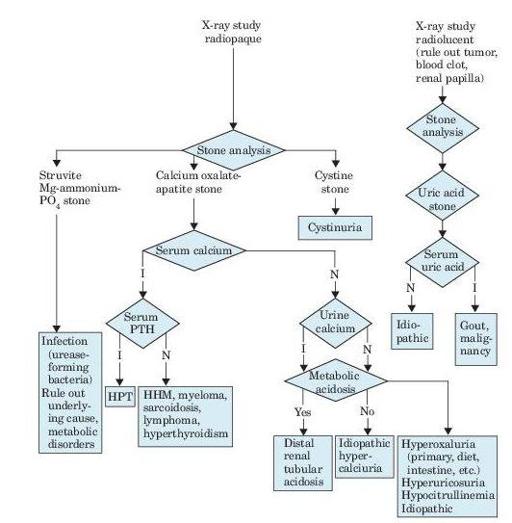
Figure 7–1
Algorithm for diagnosis of renal calculi, as revealed by flank pain, renal colic, hematuria, fever, and urinalysis findings. I, increased; N, normal; PTH, parathyroid hormone; HPT, hyperparathyroidism; HHM, humeral hypercalcemia of malignancy.
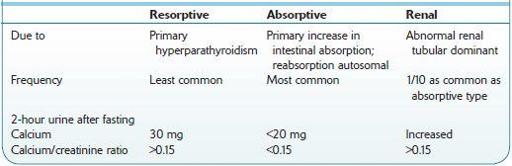
Table 7-1 Comparison of Types of Idiopathic Hypercalciuria
Who Should Be Suspected?
The waves or paroxysms of pain usually last 20–60 minutes and is related to the passage of the stone down the ureter and the associated ureteral spasm.
Other books
Two For The Lions by Lindsey Davis
Anita Blake 15 - The Harlequin by Laurell K. Hamilton
All Fired Up (Kate Meader) by Kate Meader
No Way Out by Franklin W. Dixon
Erotica from Penthouse by Marco Vassi
Bedlam Burning by Geoff Nicholson
In Other Worlds by Sherrilyn Kenyon
Seeding Her Womb: Book 1 (Alien Tentacle Erotica) by Chelsea Chaynes
BEG 1 by Kristina Weaver
Porter by Dahners, Laurence