Wallach's Interpretation of Diagnostic Tests: Pathways to Arriving at a Clinical Diagnosis (222 page)
Authors: Mary A. Williamson Mt(ascp) Phd,L. Michael Snyder Md

2. Beta-HCG level: It should be obtained to exclude pregnancy.
3. Serum TSH: For the evaluation of hyper- or hypothyroidism.
4. Consider a workup for less common endocrinopathies such as Cushing syndrome and acromegaly after excluding more common causes and only if history and physical findings raise clinical suspicion.
Imaging Studies
High-resolution CT scan or MRI is useful for localization of pituitary tumors.
Suggested Readings
Golshan M, Iglehart D. Nipple discharge. In: Rose B, (ed).
UpToDate
, Waltham, MA: UpToDate, Inc.; 2009.
Khan F, Sachs H, Pechet L, et al.
Guide to Diagnostic Testing
. Philadelphia, PA: Lippincott Williams & Wilkins; 2002.
Snyder PJ. Causes of hyperprolactinemia. In: Rose B, (ed).
UpToDate
, Waltham, MA: UpToDate, Inc.; 2009.
Snyder PJ. Clinical manifestations and diagnosis of hyperprolactinemia. In: Rose B, (ed).
UpToDate
, Waltham, MA: UpToDate, Inc.; 2009.
MALE HYPOGONADISM* (Table
6-7
)
Male hypogonadism refers to decrease in one or both testicular functions—sperm production and/or testosterone production. The root cause is either a disease of or damage to the testes (primary hypogonadism) or a disease of the pituitary or hypothalamus (secondary hypogonadism).
Table 6-7 Laboratory Diagnosis of Male Hypogonadism and Primary versus Secondary Causes
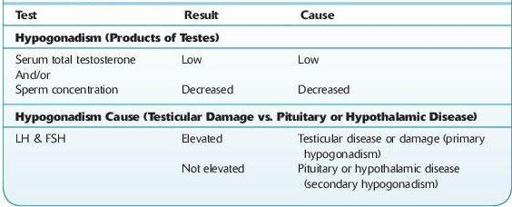
*Submitted by Charles R. Kiefer, PhD.
In general, early manifestations in postpubertal males include decreased energy and libido, whereas later manifestations include decreased androgen-dependent development of hair, muscle mass, and bone mineral density. However, there are age-related or physiologic considerations.
Manifestations in infants may include ambiguous genitalia or cryptorchidism (bearing in mind that a retractile testis usually descends into the scrotum within the first year of life). A micropenis at birth may indicate deficient gonadotropin-releasing hormone during the third trimester of pregnancy.