Wallach's Interpretation of Diagnostic Tests: Pathways to Arriving at a Clinical Diagnosis (198 page)
Authors: Mary A. Williamson Mt(ascp) Phd,L. Michael Snyder Md

BOOK: Wallach's Interpretation of Diagnostic Tests: Pathways to Arriving at a Clinical Diagnosis
6.55Mb size Format: txt, pdf, ePub
Drugs (e.g., estrogens, anabolic steroids)—most common cause (Table
5-13
)
Autosomal recessive condition; attacks begin after age 8, last weeks to months, complete resolution between episodes, may recur after months or years; exacerbated by estrogens
TABLE 5–13. Comparison of Various Types of Cholestatic Disease
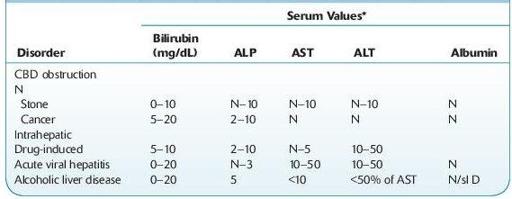
CBD, common bile duct; N, normal; sl D, slightly decreased.
*Serum value, times normal.
Laboratory Findings
Core laboratory
: Increased serum ALP, but GGT is usually normal. Serum direct bilirubin may be normal or ≤10 mg/dL. Transaminase usually <100 U.
Histology
: Liver biopsy shows centrolobular cholestasis without inflammation, bile pigment in hepatocytes and canaliculi; little or no fibrosis.
CIRRHOSIS, PRIMARY BILIARY (CHOLANGIOLITIC CIRRHOSIS, HANOT HYPERTROPHIC CIRRHOSIS, CHRONIC NONSUPPURATIVE DESTRUCTIVE CHOLANGITIS, ETC.)
Other books
The Palomino Pony Comes Home by Olivia Tuffin
Undergardeners by Desmond Ellis
River of Spears (Kingdom's Forge Book 0) by Kade Derricks
Death Benefits by Sarah N. Harvey
The Cross and the Curse (Bernicia Chronicles Book 2) by Matthew Harffy
Hunted by Heather Atkinson
Cabo Trafalgar by Arturo Pérez-Reverte
Shattered: A Psychic Visions Novel by Dale Mayer
The Honeymoon Arrangement by Wood, Joss
Christmas With Mr Darcy by Victoria Connelly