Wallach's Interpretation of Diagnostic Tests: Pathways to Arriving at a Clinical Diagnosis (136 page)
Authors: Mary A. Williamson Mt(ascp) Phd,L. Michael Snyder Md

BOOK: Wallach's Interpretation of Diagnostic Tests: Pathways to Arriving at a Clinical Diagnosis
6.4Mb size Format: txt, pdf, ePub
Structural (e.g., diaphragmatic hernia, jejunal atresia, volvulus, intestinal malrotation) Peritonitis caused by GI tract perforation, congenital infection (e.g., syphilis, TORCH [
t
oxoplasmosis,
o
ther agents,
r
ubella,
C
MV, and
h
erpes simplex], hepatitis), meconium peritonitis
M1
gangliosidosis type I, I-cell disease, β-glucuronidase deficiency)
Immune (maternal antibodies reacting to fetal antigens [e.g., Rh, C, E, Kell])
PERITONITIS, ACUTE
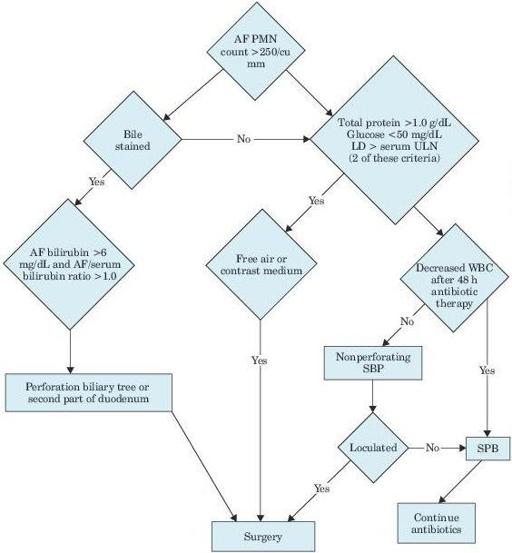
Figure 5–3
Algorithm for differentiating secondary from spontaneous bacterial peritonitis. AF, ascitic fluid; PMN, polymorphonuclear leukocytes; LD, lactate dehydrogenase; ULN, upper limit of normal; WBC, white blood cell; SBP, spontaneous bacterial peritonitis.
Other books
Love Inspired Suspense January 2014 by Shirlee McCoy, Jill Elizabeth Nelson, Dana Mentink, Jodie Bailey
Trinity Fields by Bradford Morrow
Bounce by Natasha Friend
Requited (Lost Love Series) (Erotic Romance) by Lewis, Danielle
Fortune & Fame: A Novel by Victoria Christopher Murray, ReShonda Tate Billingsley
Billy and Girl by Deborah Levy
Lady Maybe by Julie Klassen
The Enforcer by Marliss Melton
Just a Flirt by Olivia Noble
Journey to Star Wars: The Force Awakens Lost Stars by Claudia Gray, Phil Noto