Trigger Point Therapy for Myofascial Pain (14 page)
Read Trigger Point Therapy for Myofascial Pain Online
Authors: L.M.T. L.Ac. Donna Finando

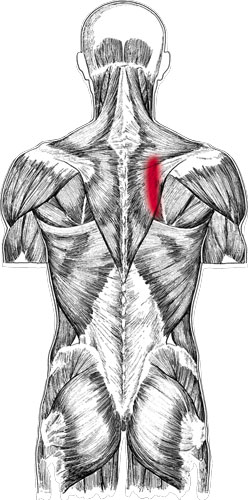
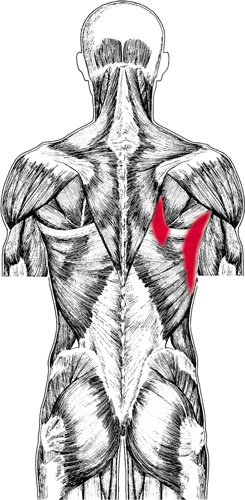
Rhomboids pain pattern
R
HOMBOIDS
R
HOMBOID
M
AJOR AND
R
HOMBOID
M
INOR
Proximal attachment:
Spinous processes of C7âT5.
Distal attachment:
Medial border of the scapula.
Action:
Elevation and retraction of the scapula.
Palpation:
To locate the rhomboids, identify the following structures:
- Medial border of the scapula
- Root of the spine of the scapulaâA small, triangular-shaped aspect of the scapula located at the medial border of the spine of the scapula. It most commonly lies on a horizontal line with T3.
- Inferior angle of the scapulaâThe sharp, triangular, distal aspect of the scapula. In most cases the inferior angle of the scapula lies on a horizontal line with T7.
- Spinous processes of C7âT5
Position the patient prone on a treatment table with his face comfortably resting in a face cradle. Ask the patient to place his hand, palm up, at the small of his back. When he pushes posteriorly against resistance provided by your hand, the rhomboids become visible.
Palpate the rhomboids between the spinal column and the medial border of the scapula, through the fibers of the trapezius muscle.
Pain pattern:
Pain concentrates along the medial border of the scapula but may spread laterally over the supraspinous area of the scapula. Local, superficial, aching pain is experienced at rest and is not influenced by movement.
Causative or perpetuating factors:
Chronic overload due to prolonged periods working in a hunched-over position; postural overload due to an overly contracted pectoralis major.
Satellite trigger points:
Levator scapulae, trapezius, infraspinatus, pectoralis major.
Affected organ system:
Respiratory system.
Associated zones, meridians, and points:
Dorsal zone; Foot Tai Yang Bladder meridian; BL 11â15, BL 41â44.
Stretch exercise:
Sit in a chair. Bend forward, dropping the head. Cross each arm over the body to grasp the opposite knee. Hold this position for a count of five to ten.
Strengthening exercise:
Lie diagonally across a bed or table, your arms hanging over the edge. Bend the elbows to 90 degrees. Retract the scapulae. Hold this position for a count of ten. Release and repeat.
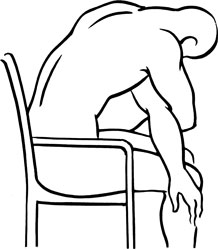
Stretch exercise: Rhomboids
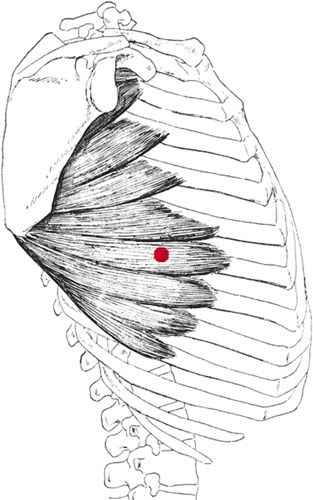
Serratus anterior and trigger point
S
ERRATUS
A
NTERIOR
Anterior attachment:
Through slips (digitations) lying on the anterolateral aspect of rib 1 through ribs 8 or 9.
Posterior attachment:
Passing deep to the scapula to attach to the costal surface of the full length of the scapula's medial border, with the heaviest attachment onto its inferior angle.
Action:
Protraction of the scapula; lateral rotation of the scapula resulting in upward rotation of the glenoid fossa; assists in upward rotation and elevation of the scapula; stabilizes the scapula against the thoracic wall during forward-pushing movements.
Palpation:
Serratus anterior, lying on the lateral aspect of the thoracic wall, forms the medial wall of the axilla. At its anterior attachment to the lower ribs, slips of this muscle interdigitate with the costal attachment of external oblique. Locate the serratus anterior with the patient lying on his side, the arm flexed and extended backward toward the surface of the table. Palpate superficially at the midaxillary line at the level of ribs 5 or 6, on the same horizontal line with the nipple. Palpate distally to ribs 8 and 9 to identify slips of the lower aspect of the serratus anterior; palpate superiorly from the midline to palpate slips of serratus anterior lying on ribs 1 through 5. Trigger points are most commonly found at the midaxillary line at the level of ribs 5 and 6. However, trigger points can develop in any of the slips (digitations) of serratus anterior.
Pain pattern:
Pain in the anterolateral aspect of the chest as well as the medial to the inferior angle of the scapula. Pain may radiate down the ulnar surface of the homolateral arm and may extend as far as the palm and the ring finger. Symptoms include pain that is persistent, intense, and unaffected by movement or position; shortness of breath or the inability to take a deep breath without pain; inability to expand the lower chest during inspiration; breast or nipple pain.
Causative or perpetuating factors:
Fast or prolonged running, push-ups, overhead lifting, chin-ups, severe coughing.
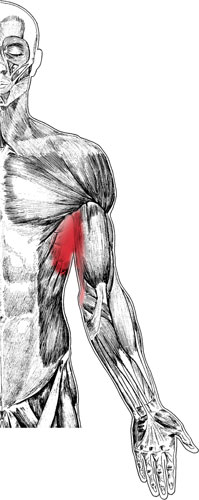
Serratus anterior pain pattern
Satellite trigger points:
Latissimus dorsi, scalenes, and sternocleidomastoid (the accessory muscles of breathing).
Affected organ systems:
Respiratory and digestive systems.
Associated zones, meridians, and points:
Lateral zone; Hand Tai Yin Lung meridian, Foot Tai Yin Spleen meridian, Foot Shao Yang Gall Bladder meridian; SP 21, GB 22 and 23.
Stretch exercises:
1.   Sitting on a chair, place the arm of the affected side over the back of the chair and hold the seat of the chair behind you. Using that arm to fix your shoulder blade, slowly turn your thorax in the opposite directionâfor example, if the painful side is your left side, hold the back of the chair with your left arm and turn your torso toward the right.
2.   Lower and middle positions of the doorway stretchâsee page 81: With the forearms placed firmly on each side of a doorway, stretch the body through the outstretched arms, opening the chest and anterior shoulder region. Position 1: place the palms approximately at ear level. Position 2: place the elbows level with the shoulders.
Strengthening exercise:
No strengthening exercise is needed due to the nature of this muscle.

Stretch exercise: Serratus anterior
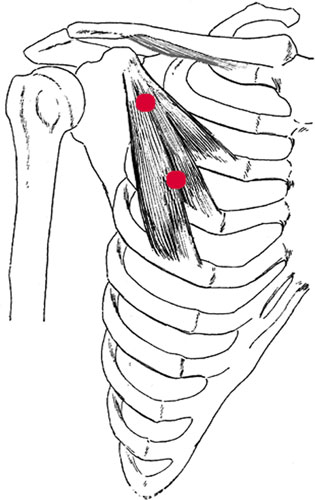
Pectoralis minor and trigger points
P
ECTORALIS
M
INOR
Proximal attachment:
Coracoid process of the scapula.
Distal attachment:
Anterior chest wall, on the upper surfaces of ribs 3, 4, and 5.
Action:
Pulls the scapula and shoulder down and forward; assists in forced inspiration.
Palpation:
Pectoralis minor lies deep to pectoralis major and may be difficult to palpate. During palpation the two pectoralis muscles may be differentiated by the direction of their fibers.
To locate pectoralis minor, identify the following structures:
- Coracoid process of the scapulaâProjecting anteriorly from the superior border of the head of the scapula. Find the most concave aspect of the lateral clavicle; move your palpating hand distally approximately 1 inch into the deltopectoral triangle. Pressing posterolaterally, you will feel the coracoid process as a bony prominence. This area can be quite sensitive.
- Ribs 2 through 5âLocate the sternal articulations of ribs 2 through 5. Follow the course of each rib and rib space from the sternum toward the shoulder, noting the upward contours of the ribs as you palpate laterally. Note that rib 1 lies under the clavicle and so cannot be easily distinguished through palpation. Rib 2 is the first distinctly palpable rib distal to the clavicle.