Surviving the Medical Meltdown (23 page)
Read Surviving the Medical Meltdown Online
Authors: Lee Hieb

This is not a daily iodine supplement but a larger dose of iodine to prevent thyroid cancer when exposed to radiation, as happened to people near Fukushima and Chernobyl. Taken before the exposure, it is highly effective, and it is still 90 percent effective within two hours of exposure. Although the effectiveness degrades with time, because there is a risk of some ongoing exposure, I would take a single dose even a day or so after exposure. Generally take one dose as soon as a significant risk is known, and in prolonged exposure a daily dose for three days may be warranted – except in neonates and breast-feeding women. Keep in mind that adults over forty have less chance of thyroid cancer than younger people and a greater chance of allergy to KI. In the event of a radiation emergency, hopefully you will have some official source of information, but generally the government is too slow, in denial, and more worried about damage control for itself than damage control for you. Here are the dosing guidelines – understand that early action is best.

*
Adolescents approaching adult size (≥70 kg) should receive the full adult dose (130 mg).
**
FDA understands that a KI administration program that sets different projected thyroid radioactive dose thresholds (committed dose equivalent (CDE)) for treatment of different population groups may be logistically impractical to implement during a radiological emergency.
SOURCE: Radiation Emergency Medical Management, DHS,
http://www.remm.nlm.gov/potassiumiodide.htm
Finally, let me take this opportunity to criticize the current thinking on nuclear exposure. Although the information just given is most likely to be used in the event of a nuclear power plant accident, it is dangerous to ignore the possibility of a nuclear conflict between nation-states or a nuclear weapon being detonated by a nonstate
actor, such as the current crop of terrorists. Although comedians and various talking heads make fun of the old nuclear drills done in the 1960s, the principles taught back then make sense and will save lives. (Many people think, mistakenly, that the chance of surviving is so low there is no reason to worry about learning such precautions.) In short, if you see a flash, drop under a desk or other object to avoid being struck by flying glass. Stay there for two minutes. Remember the 7:10 rule. Radiation loses 90 percent of its radioactivity in the first seven hours and 90 percent for every sevenfold interval of time, or 90 percent in seven hours, 99 percent in forty-nine hours, and 99.9 percent in fourteen days. Fallout looks like ash grit or sand. Place a white paper outside to check for it. No fallout, no radiation. Further information on radiation and other disaster medical preparedness can be found on the Doctors for Disaster Preparedness website, at
http://www.ddponline.org
. A handbook of emergency care in disaster scenarios can also be obtained from their site at
http://www.ddponline.org/handbookforsurvival.pdf
.
BIOLOGIC PRECAUTIONS
Unfortunately, although we may have reduced death from many childhood diseases, the world is an increasingly dangerous place. We may not be dying of malaria in the United States, but we are facing new threats from biologic agents of war and from the diseases being reintroduced by the hordes of illegal immigrants currently coming up from Central America. For these issues you need to be prepared for medical isolation if necessary.
BIOTERRORISM
After 9/11, I decided to educate myself about bioterrorism because my county health department spent $250,000 on a decontamination unit. My question was, what are they expecting to decontaminate? After enough research that I became a speaker on this topic, most recently giving a presentation to Doctors for Disaster Preparedness,
I still don’t know what they planned on decontaminating. But I did learn there are some real issues out there, and we are sticking our collective national head in the sand.
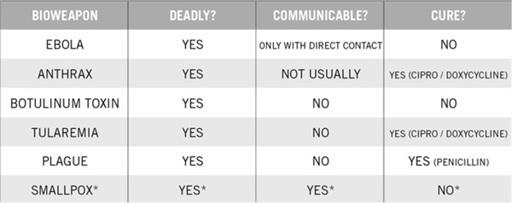
The Obama administration, which claims to be the smartest group of political geniuses ever to grace the halls of American power, just got an F – for “Fail” – from Homeland Security for their inability to defend us against chemical or biologic attack. I, for one, was not surprised. For years I attempted to rouse then governor of Arizona Janet Napolitano to the dangers of biologic attack, and received no response. Failing at algebra is one thing, but the consequences of this failing grade could be the destruction of America and any other nation with its head in the sand on this issue. There are a handful of biologic agents that can be used as effective weapons. In most cases, either there is a treatment (such as with anthrax) or the disease is unlikely to spread (as with the botulinum toxin) or it is debilitating in the short term but not terribly deadly (in the case of salmonella). If, however, you want to pick a biologic agent that is very deadly, very communicable, and for which no treatment exists, you want smallpox.
SMALLPOX
The United States stopped routine smallpox vaccinations in 1972, the last known natural case occurring in 1967. Smallpox is an unbelievably deadly disease. It is the most contagious disease known to mankind – spreading literally like smoke. In the last known outbreak in Europe, a man early in the throes of smallpox, against doctor’s advice, opened his hospital window. In the cold German night, his exhalations went out the window, up the hospital wall, into an open window on another wing, and killed several nurses. That’s contagious.
Smallpox is a virus for which there is no known treatment, and in some outbreaks the death rate for those infected was over 60 percent. Modern medicine brought the contagion under control by a process of “ring vaccination.” The Centers for Disease Control
(CDC), the World Health Organization (WHO), and other agencies prepositioned vaccine at hot spots all over the world. They had trained teams of medical personnel ready to go at a moment’s notice to fly to any area suffering an outbreak and begin vaccinating people in a ring around the incident case until the outbreak stopped.
While it is true that smallpox has been eradicated in the wild, it is not gone. As smallpox came under some control, samples from the disease were given to the CDC in Atlanta and to Biopreparat/Vector in the Soviet Union. Just as Oppenheimer thought it would be a more stable world if both sides had nuclear bombs, the WHO thought it was only fair that both the democratic United States and the totalitarian Soviets should have samples of the world’s deadliest disease.
We know for a fact that when Nixon signed the treaty with the Soviets in the early 1970s to halt all offensive bioweapons research and deployment, the Russians went right home and created the largest bioweapons program known to mankind. According to Ken Alibek (his Americanized name), himself a defector and the number-two man at Vector State Research Center of Virology and Biotechnology, the Soviet Union had vats filled with more than twenty tons of India-11 smallpox that had been prepared for delivery in warheads. Our intelligence services had witnessed testing of ICBM reentry vehicles with nose-cone cooling, something needed only for bioagents. And we know that at the fall of the Soviet empire, the bioweaponeers disappeared, along with their agents – presumably to the highest bidder.
So here is the scenario in a nutshell. Smallpox virus survives in freezers all over the world – not just in friendly hands. We found incubation vats in Iraq labeled “smallpox,” and we captured Saddam’s bioweaponeer, a woman fondly referred to as Dr. Germ. The virus that was manufactured by the Soviets was about 60 percent lethal, and the amount to start a worldwide contagion may be stored in a single chicken egg. Before, disease containment was possible because (1) much of the developed world was vaccinated, (2) teams trained to handle outbreaks were standing by for ready deployment
worldwide, (3) vaccine was stashed in accessible depots all over the world, (4) populations were less mobile, and (5) people knew not to go to hospitals during smallpox outbreaks but to allow a system of quarantine. But today, none of these things is true; and additionally, since the 1970s, we have the scientific wherewithal to genetically modify (weaponize) the virus.
I served in the military and have had a number of smallpox vaccinations. Unfortunately, these probably last only fifteen years. As a trauma surgeon and emergency responder, I tried to be voluntarily vaccinated but was turned down. At that time, Janet Reno was governor of Arizona, and she was worried that voluntary vaccination of hospital personnel might result in workman’s compensation claims. How do you spell shortsighted? Since 9/11, I have written to two governors and numerous health agencies, expressing my fear about the deadliest terrorist weapon – biologic agents, particularly smallpox. My request was a simple one – let the first responders be voluntarily inoculated against smallpox. At present only a handful of people in county health departments are vaccinated.
*
Only smallpox is deadly, communicable, and without cure.
So, in the case of a bioweapon being released, to be prepared, first you need to be knowledgeable because the news will not tell you the whole or even the true story should this occur. Don’t panic
for outbreaks of influenza, anthrax, ebola, or pretty much any other bioterrorist weapon – unless you hear the word
smallpox
. If there is even one case of smallpox reported anywhere in the world, it is cause for action. The only action you can take is to isolate yourself. I have told my family that should smallpox break out anywhere in the world, within days of the report it will be global. Do not get on any public transportation. It is time to get to a freestanding domicile, preferably a rural one, that has enough supplies to last several months. I won’t repeat classic survivalist instruction here, but suffice it to say that this is the one situation in which secure isolation is the safest solution. You cannot allow any potentially contaminated people near you. I hope that public health will be able to distribute the vaccine and that there will be house-to-house vaccination or some other sort of community vaccination program. Keep in mind that vaccination pre-exposure is essentially 100 percent effective in preventing the disease. Vaccination after exposure mitigates death but does not completely diminish the chance of contracting this disfiguring disease. In your stored medications I have recommended both cipro and doxicycline as treatment. Most masks will not screen out smallpox, but they may help with other communicable diseases such as TB (see below). For this purpose you should have a box of N95 masks in appropriate sizes, and keep them at home, in your car, and in your emergency kits.
Illegal immigrants
now swarming the southern border from El Salvador, Honduras, and Guatemala are bringing with them a panoply of diseases that, up until now, have been rare in the United States or had been eradicated. Although legal immigration required testing for a number of communicable diseases, illegals gain entry without any such precaution. If unchecked, this latest assault on our border integrity will become not only a crime problem but a public health disaster.
DISEASES OF ILLEGAL IMMIGRATION
1.
Multidrug-resistant TB
2.
Chagas disease
3.
Leprosy
4.
Measles
5.
Influenza
6.
Malaria
7.
Dengue fever
8.
Hepatitis A, B, C, E
9.
Lice, scabies, and other parasites
Tuberculosis (TB)
was once very common but had been controlled in the United States through testing and public health measures. Prior to anti-TB meds, 2 percent of medical students died during training due to patient exposure to the disease. Today about two million people worldwide die yearly from TB, and now we are facing an influx of the very worst strain of the disease brought in through illegal immigration. Multiple-drug-resistant TB requires very expensive medications to be given – often through IV – sometimes for years. Even so, it carries a 50 percent chance of premature death and costs from $250,000 to $1.2 million to treat one patient. Currently, a good number of the immigrants reaching and crossing the border are sick with one or more of these diseases. They are coughing up blood, and they are malnourished and infested with body lice and parasites. The border patrol agents trying to control the problem are being infected.
1
At the time of this writing, the nationwide impact of this disaster has yet to play out, so clear recommendations are difficult. In general, optimize your vitamin D levels and
your general health to be resistant to disease as much as possible. Keep N95 masks – which were designed specifically to filter out TB particles – handy for unexpected situations. Keep cipro and doxicycline in your medical stores, along with treatment for lice (Quell). If you are going to be hospitalized, especially if this is elective and you have the luxury of rescheduling, ask about cases of TB and whether or not such cases are in the hospital. The sad fact is, in the old days we had sanatoriums where we isolated TB victims and applied “open-air treatment.” These are all closed. Today, modern non-research hospitals rarely have true isolation rooms. They can put the TB patient into a single-bed room, but the air that circulates through the room also circulates around into other patients’ rooms. So having your gall bladder surgery could get you exposed to a bad disease – if this crisis spreads.